

SARS-CoV-2, influenza A/B and respiratory syncytial virus positivity and association with influenza-like illness and self-reported symptoms, over the 2022/23 winter season in the UK: a longitudinal surveillance cohort
- PMID: 38532381
- PMCID: PMC10964495
- DOI: 10.1186/s12916-024-03351-w
SARS-CoV-2, influenza A/B and respiratory syncytial virus positivity and association with influenza-like illness and self-reported symptoms, over the 2022/23 winter season in the UK: a longitudinal surveillance cohort
Abstract
Background: Syndromic surveillance often relies on patients presenting to healthcare. Community cohorts, although more challenging to recruit, could provide additional population-wide insights, particularly with SARS-CoV-2 co-circulating with other respiratory viruses.
Methods: We estimated the positivity and incidence of SARS-CoV-2, influenza A/B, and RSV, and trends in self-reported symptoms including influenza-like illness (ILI), over the 2022/23 winter season in a broadly representative UK community cohort (COVID-19 Infection Survey), using negative-binomial generalised additive models. We estimated associations between test positivity and each of the symptoms and influenza vaccination, using adjusted logistic and multinomial models.
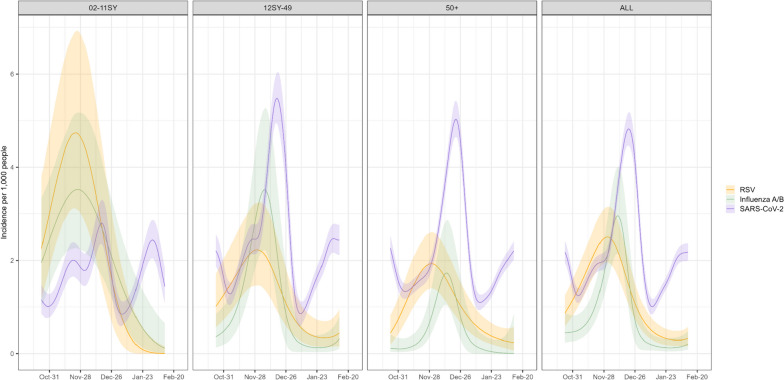
Results: Swabs taken at 32,937/1,352,979 (2.4%) assessments tested positive for SARS-CoV-2, 181/14,939 (1.2%) for RSV and 130/14,939 (0.9%) for influenza A/B, varying by age over time. Positivity and incidence peaks were earliest for RSV, then influenza A/B, then SARS-CoV-2, and were highest for RSV in the youngest and for SARS-CoV-2 in the oldest age groups. Many test positives did not report key symptoms: middle-aged participants were generally more symptomatic than older or younger participants, but still, only ~ 25% reported ILI-WHO and ~ 60% ILI-ECDC. Most symptomatic participants did not test positive for any of the three viruses. Influenza A/B-positivity was lower in participants reporting influenza vaccination in the current and previous seasons (odds ratio = 0.55 (95% CI 0.32, 0.95)) versus neither season.
Conclusions: Symptom profiles varied little by aetiology, making distinguishing SARS-CoV-2, influenza and RSV using symptoms challenging. Most symptoms were not explained by these viruses, indicating the importance of other pathogens in syndromic surveillance. Influenza vaccination was associated with lower rates of community influenza test positivity.
Keywords: Influenza a/b; Influenza-like illness; Respiratory syncytial virus; SARS-CoV-2; Surveillance; Symptoms; Vaccination.
© 2024. The Author(s).
Conflict of interest statement
DWE declares lecture fees from Gilead, outside the submitted work. PCM has received GSK funding support.
Figures



References
-
- Shi T, Denouel A, Tietjen AK, Campbell I, Moran E, Li X, et al. Global disease burden estimates of respiratory syncytial virus-associated acute respiratory infection in older adults in 2015: a systematic review and meta-analysis. J Infect Dis. 2020;222(Supplement 7):S577–S583. doi: 10.1093/infdis/jiz059. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
