

Symptoms and quality of life among men starting treatment for metastatic castration-resistant prostate cancer - a prospective multicenter study
- PMID: 38532425
- PMCID: PMC10967147
- DOI: 10.1186/s12904-024-01410-w
Symptoms and quality of life among men starting treatment for metastatic castration-resistant prostate cancer - a prospective multicenter study
Abstract
Background: Men with metastatic castration-resistant prostate cancer (mCRPC) have an incurable disease. Along with prolonging life, symptom management is one of the main goals with treatment. This is also important from a palliative care perspective where the life prolonging outcomes should be balanced with quality of life (QoL) in this late phase. It is also essential in symptom management to view different dimensions of symptoms, for example how severe or distressing symptoms are, to support best QoL. Therefore, more knowledge is needed about the symptom experience when these treatments are initiated and thus the aim of this study was to describe different dimensions of symptoms in men with mCRPC starting their first-line of life-prolonging treatment, and to describe the association between symptom burden and QoL.
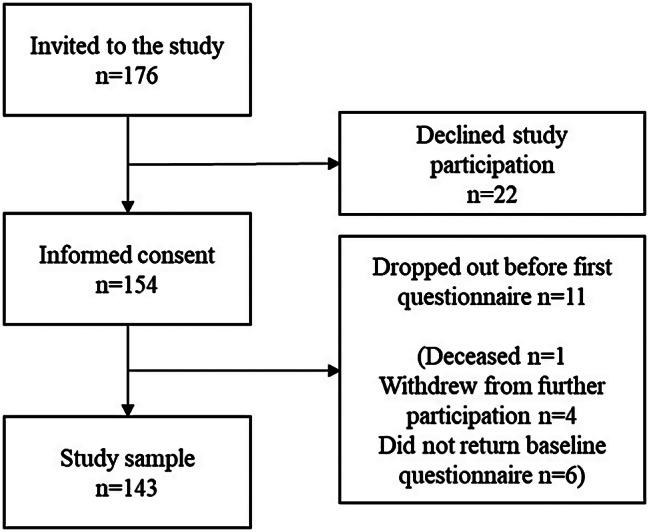
Methods: Baseline data from a prospective longitudinal study of 143 men with mCRPC starting their first-line life-prolonging treatment were used. Symptoms were measured using the Memorial Symptom Assessment Scale (MSAS) and global QoL was measured by the EORTC QLQ C-30. Data was analyzed using descriptive- and multivariable linear regression analyses.
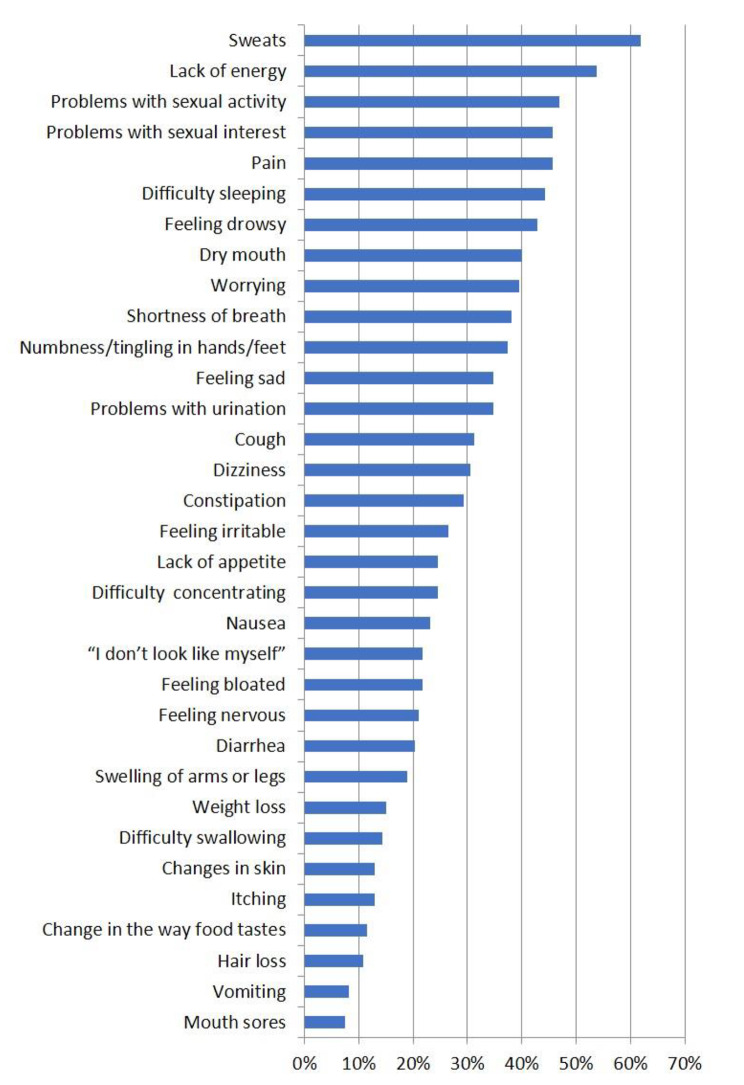
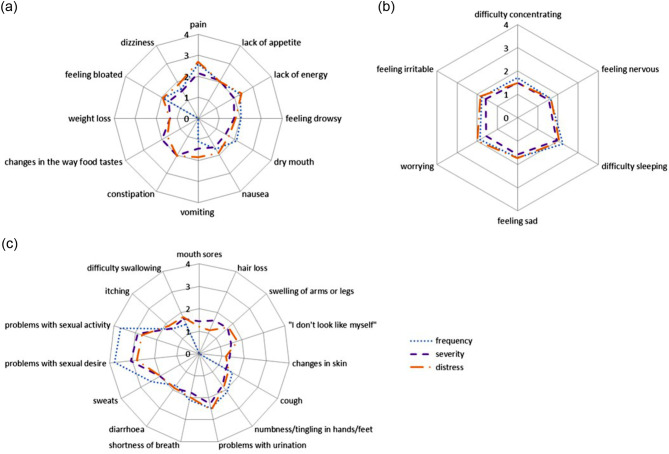
Results: On average, the men had more than 10 symptoms (range 0-31 of 33). 50% or more reported sweats, lack of energy, pain, problems with sexual activity and sexual desire. The symptoms they reported as most severe, or most distressing were not always the ones that were reported as most frequent. There was an association between QoL and physical symptoms, and also between QoL, and analgesic use and prostate-specific antigen (PSA) values.
Conclusion: Even if some men with mCRPC report many symptoms, the dimensions of severity and distress levels vary, and the most frequent symptoms was not always the most burdensome or distressing. There was an association between high physical symptom burden and QoL, suggesting that it is not the number of symptoms that affects QoL but rather the subjective perceived impact of the physical symptoms experienced. The knowledge of how men with mCRPC experience and perceive their symptoms may help health care professionals in symptom management aiming to improve QoL, which is a cornerstone in integrating early palliative care.
Keywords: Early integrated palliative care; MSAS; Metastatic castration-resistant prostate cancer; Prostatic neoplasm; Quality of life; Symptom burden; Symptom management.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Symptom burden among men treated for castration-resistant prostate cancer: a longitudinal study.BMJ Support Palliat Care. 2024 Dec 25;15(1):87-95. doi: 10.1136/spcare-2024-005054. BMJ Support Palliat Care. 2024. PMID: 39122263 Free PMC article.
-
The role of frailty in modifying physical function and quality of life over time in older men with metastatic castration-resistant prostate cancer.J Geriatr Oncol. 2023 Mar;14(2):101417. doi: 10.1016/j.jgo.2022.12.005. Epub 2023 Jan 20. J Geriatr Oncol. 2023. PMID: 36682218
-
Impact of treatment on elder-relevant physical function and quality of life outcomes in older adults with metastatic castration-resistant prostate cancer.J Geriatr Oncol. 2023 Jan;14(1):101395. doi: 10.1016/j.jgo.2022.10.010. Epub 2022 Oct 28. J Geriatr Oncol. 2023. PMID: 36988103
-
Health-related quality of life in men with metastatic castration-resistant prostate cancer.Expert Rev Pharmacoecon Outcomes Res. 2015;15(6):941-9. doi: 10.1586/14737167.2015.1107479. Epub 2015 Oct 29. Expert Rev Pharmacoecon Outcomes Res. 2015. PMID: 26512743 Review.
-
Telephone interventions for symptom management in adults with cancer.Cochrane Database Syst Rev. 2020 Jun 2;6(6):CD007568. doi: 10.1002/14651858.CD007568.pub2. Cochrane Database Syst Rev. 2020. PMID: 32483832 Free PMC article.
Cited by
-
Patient, caregiver experiences in metastatic castration-resistant prostate cancer: insights from a multi-national survey.Future Oncol. 2025 Jul;21(16):2053-2066. doi: 10.1080/14796694.2025.2510890. Epub 2025 Jun 2. Future Oncol. 2025. PMID: 40452494 Free PMC article.
References
-
- Ryan CJ, Smith MR, Fizazi K, Saad F, Mulders PF, Sternberg CN, et al. Abiraterone acetate plus prednisone versus placebo plus prednisone in chemotherapy-naive men with metastatic castration-resistant prostate cancer (COU-AA-302): final overall survival analysis of a randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol. 2015;16(2):152–60. doi: 10.1016/S1470-2045(14)71205-7. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
