

Hot avulsion versus argon plasma coagulation for the management of the non-ensnarable polyp: A multicenter, randomized controlled trial
- PMID: 38533237
- PMCID: PMC10964916
- DOI: 10.1002/jgh3.13052
Hot avulsion versus argon plasma coagulation for the management of the non-ensnarable polyp: A multicenter, randomized controlled trial
Abstract
Background and aim: Snare resection of nonlifting colonic lesions often requires supplemental techniques. We compared the success rates of neoplasia eradication using hot avulsion and argon plasma coagulation in colonic polyps when complete snare polypectomy had failed.
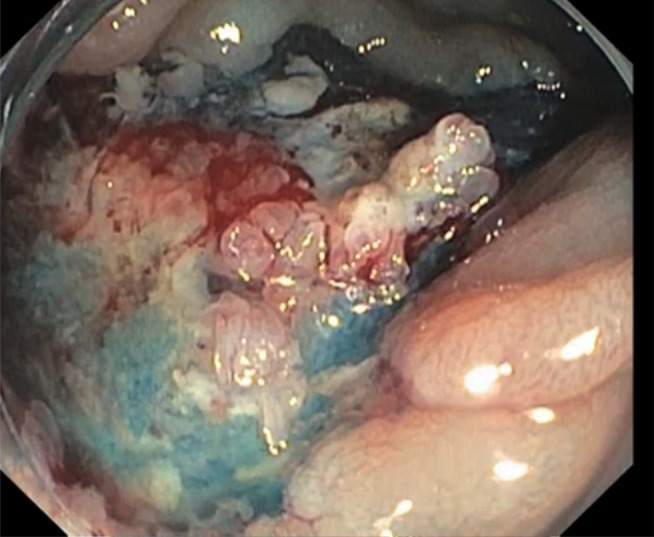
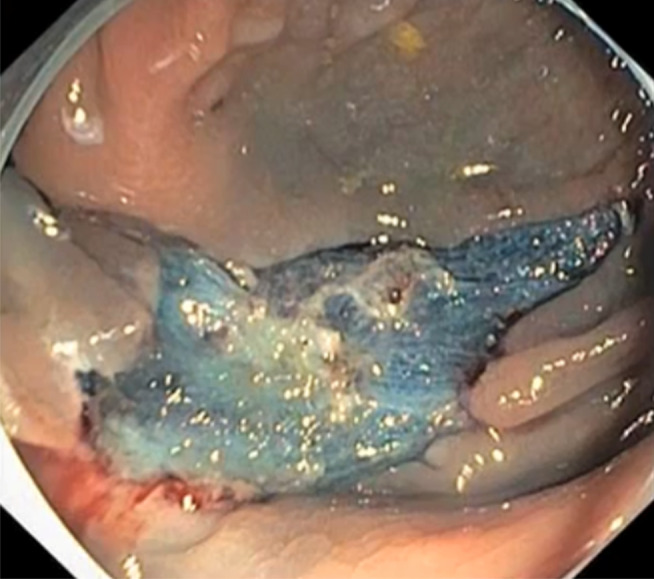
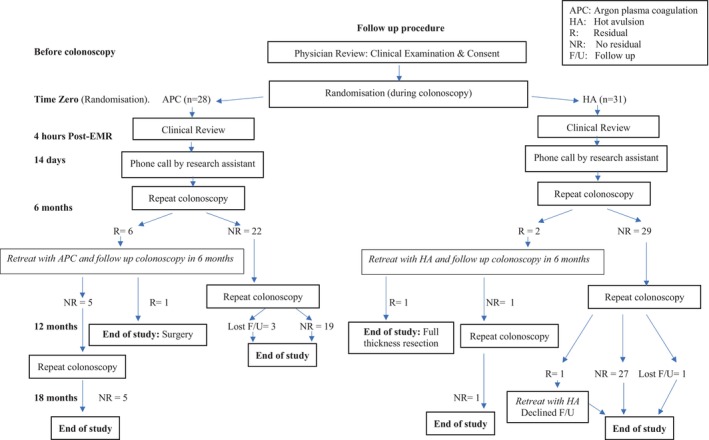
Methods: Polyps that were not completely resectable by snare polypectomy were randomized to argon plasma coagulation or hot avulsion for completion of resection. Argon plasma coagulation was delivered using a forward shooting catheter, using a nontouch technique (flow 1.2 L, 35 watts). Hot avulsion was performed by grasping the neoplastic tissue with hot biopsy forceps and applying traction away from the bowel wall while using EndoCut I or soft coagulation for avulsion. Surveillance colonoscopies were performed at 6, 12, and 18 months.
Results: From November 2013 to July 2017, 59 patients were randomized to argon plasma coagulation (28) or hot avulsion (31). The median age was 69 (60-75), with 46% being female. The median residual tissue size was 10 mm (6-12). The residual adenoma rate at 6 months (hot avulsion 6% vs argon plasma coagulation 21% P = 0.09) and 18 months was not different between the groups (6.6% vs 3.6% P = 0.25). One patient in the argon plasma coagulation arm was diagnosed with metastatic cancer of likely colorectal origin despite benign histology in the original polypectomy specimen, supporting the importance of tissue acquisition.
Conclusion: Both hot avulsion and argon plasma coagulation are effective and safe modalities to complete resection of non-ensnarable colonic polyps.
Keywords: argon plasma coagulation; hot avulsion; polypectomy.
© 2024 The Authors. JGH Open published by Journal of Gastroenterology and Hepatology Foundation and John Wiley & Sons Australia, Ltd.
Figures
Similar articles
-
Cold snare polypectomy vs. hot snare polypectomy vs. argon plasma coagulation for small (5-9mm) left-sided colorectal polyps: a prospective randomized trial.Eur J Gastroenterol Hepatol. 2021 Dec 1;33(1S Suppl 1):e909-e915. doi: 10.1097/MEG.0000000000002300. Eur J Gastroenterol Hepatol. 2021. PMID: 35048657 Clinical Trial.
-
Large sessile colonic adenomas: use of argon plasma coagulator to supplement piecemeal snare polypectomy.Gastrointest Endosc. 1999 Jun;49(6):731-5. doi: 10.1016/s0016-5107(99)70291-9. Gastrointest Endosc. 1999. PMID: 10343218
-
Avulsion is superior to argon plasma coagulation for treatment of visible residual neoplasia during EMR of colorectal polyps (with videos).Gastrointest Endosc. 2016 Nov;84(5):822-829. doi: 10.1016/j.gie.2016.03.1512. Epub 2016 Apr 11. Gastrointest Endosc. 2016. PMID: 27080417
-
AGA Clinical Practice Update on Appropriate and Tailored Polypectomy: Expert Review.Clin Gastroenterol Hepatol. 2024 Mar;22(3):470-479.e5. doi: 10.1016/j.cgh.2023.10.012. Epub 2023 Nov 28. Clin Gastroenterol Hepatol. 2024. PMID: 38032585 Review.
-
Effectiveness and safety of cold versus hot snare polypectomy: A meta-analysis.J Gastroenterol Hepatol. 2019 Jan;34(1):49-58. doi: 10.1111/jgh.14464. Epub 2018 Sep 26. J Gastroenterol Hepatol. 2019. PMID: 30176072
References
-
- Moss A, Bourke M, Williams S et al. Endoscopic mucosal resection outcomes and prediction of submucosal cancer from advanced colonic mucosal neoplasia. Gastroenterology. 2011; 140: 1909–1918. - PubMed
-
- Salama M, Ormonde D, Quach T, Ee H, Yusoff I. Outcomes of endoscopic resection of large colorectal neoplasms: an Australian experience. J. Gastroenterol. Hepatol. 2010; 25: 84–89. - PubMed
-
- Tate D, Bahin F, Desomer L, Sidhu M, Gupta V, Bourke M. Cold‐forceps avulsion with adjuvant snare‐tip soft coagulation (CAST) is an effective and safe strategy for the management of non‐lifting large laterally spreading colonic lesions. Endoscopy. 2018; 50: 52–62. - PubMed
-
- Ferlitsch M, Moss A, Hassan C et al. Colorectal polypectomy and endoscopic mucosal resection (EMR): European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy. 2017; 49: 270–297. - PubMed
LinkOut - more resources
Full Text Sources
