

Risk of Death and Cardiovascular Events in Asian Patients With Atrial Fibrillation and Chronic Obstructive Pulmonary Disease: A Report From the Prospective APHRS Registry
- PMID: 38533983
- PMCID: PMC11179754
- DOI: 10.1161/JAHA.123.032785
Risk of Death and Cardiovascular Events in Asian Patients With Atrial Fibrillation and Chronic Obstructive Pulmonary Disease: A Report From the Prospective APHRS Registry
Abstract
Background: Chronic obstructive pulmonary disease (COPD) is associated with an increased risk of adverse events in patients with atrial fibrillation (AF); however, few data are available on this topic in Asian populations.
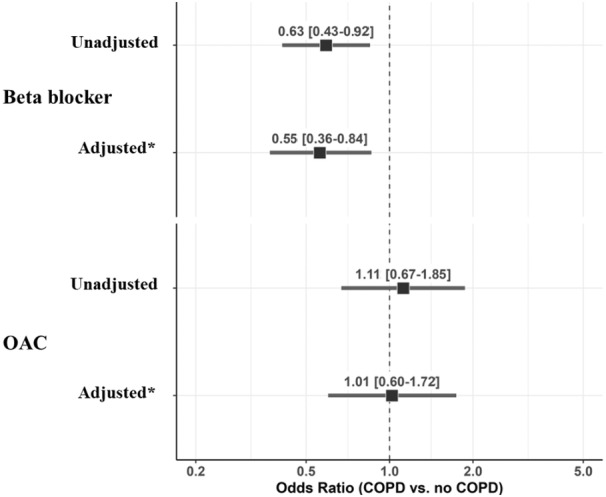
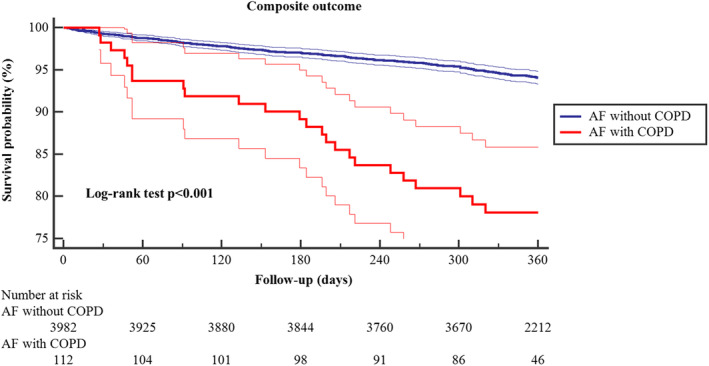
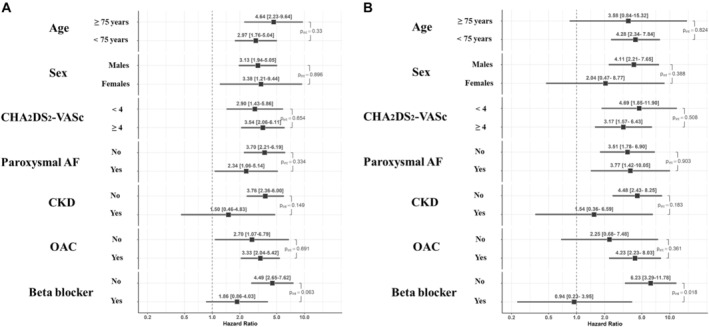
Methods and results: Prospective observational study conducted on patients with AF enrolled in the Asia-Pacific Heart Rhythm Society (APHRS) AF Registry. The diagnosis of COPD was based on data reported in the case report form by the investigators. Cox-regression models were used to assess the 1-year risk of a primary composite outcome of all-cause death, thromboembolic events, acute coronary syndrome, and heart failure. Analysis on single outcomes and cardiovascular death was also performed. Interaction analysis was used to assess the risk of composite outcome and all-cause death in different subgroups. The study included 4094 patients with AF (mean±SD age 68.5±12 years, 34.6% female), of whom 112 (2.7%) had COPD. Patients with COPD showed a higher incidence of the primary composite outcome (25.1% versus 6.3%, P<0.001), all-cause death (14.9% versus 2.6%, P<0.001), cardiovascular death (2.0% versus 0.6%, P<0.001), and heart failure (8.3% versus 6.0%, P<0.001). On multiple Cox-regression analysis, COPD was associated with a higher risk of the primary composite outcome (hazard ratio [HR], 3.17 [95% CI, 2.05-4.90]), all-cause death (HR, 3.59 [95% CI, 2.04-6.30]), and heart failure (HR, 3.32 [95% CI, 1.56-7.03]); no statistically significant differences were found for other outcomes. The association between COPD and mortality was significantly modified by the use of beta blockers (Pint=0.018).
Conclusions: In Asian patients with AF, COPD is associated with worse prognosis. In patients with AF and COPD, the use of beta blockers was associated with a lower mortality.
Registration information: clinicaltrials.gov Identifier: NCT04807049.
Keywords: COPD; all‐cause death; atrial fibrillation; beta blockers; heart failure.
Figures
References
-
- Pokorney SD, Piccini JP, Stevens SR, Patel MR, Pieper KS, Halperin JL, Breithardt G, Singer DE, Hankey GJ, Hacke W, et al. Cause of death and predictors of all‐cause mortality in anticoagulated patients with nonvalvular atrial fibrillation: data from ROCKET AF. J Am Heart Assoc. 2016;5:e002197. doi: 10.1161/JAHA.115.002197 - DOI - PMC - PubMed
-
- Romiti GF, Corica B, Pipitone E, Vitolo M, Raparelli V, Basili S, Boriani G, Harari S, Lip GYH, Proietti M, et al. Prevalence, management and impact of chronic obstructive pulmonary disease in atrial fibrillation: a systematic review and meta‐analysis of 4,200,000 patients. Eur Heart J. 2021;42:3541–3554. doi: 10.1093/eurheartj/ehab453 - DOI - PubMed
-
- Raparelli V, Pastori D, Pignataro SF, Vestri AR, Pignatelli P, Cangemi R, Proietti M, Davi G, Hiatt WR, Lip GYH, et al. Major adverse cardiovascular events in non‐valvular atrial fibrillation with chronic obstructive pulmonary disease: the ARAPACIS study. Intern Emerg Med. 2018;13:651–660. doi: 10.1007/s11739-018-1835-9 - DOI - PubMed
