

Suprapubic and Transurethral Bladder Access for Voiding Cystourethrography in Pediatric Male Patients
- PMID: 38535513
- PMCID: PMC10975646
- DOI: 10.3390/pediatric16010017
Suprapubic and Transurethral Bladder Access for Voiding Cystourethrography in Pediatric Male Patients
Abstract
Purpose: To compare suprapubic access (SPA) and transurethral catheterization (TUC) in voiding cystourethrogram (VCUG).
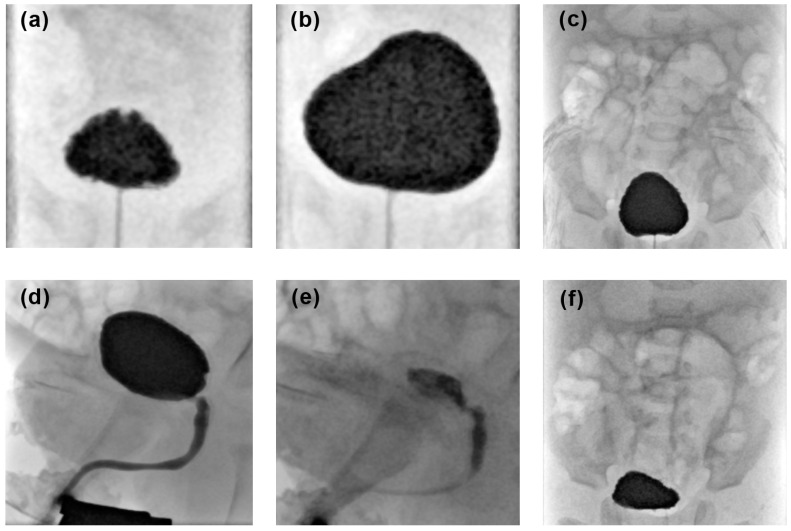
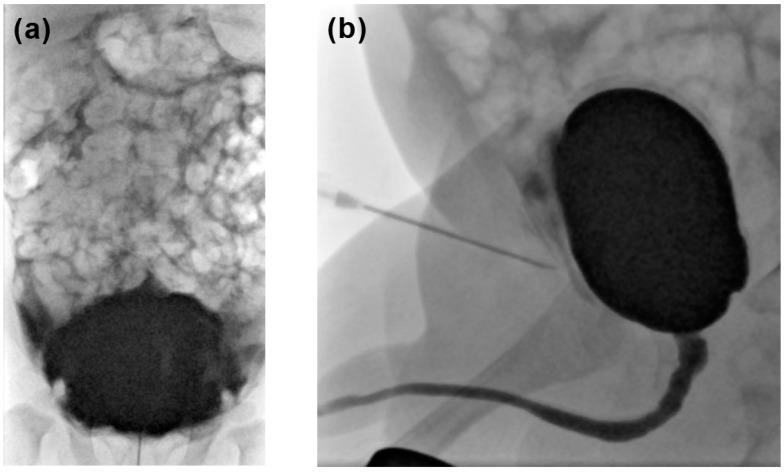
Methods: Retrospective single-center evaluation of 311 VCUG performed in male patients under 12 years of age. Two study groups were built based on the bladder access method. TUC was performed in 213 patients, whereas 98 received SPA. The groups were compared regarding the procedural switch rate, the complication rate, radiation parameters, the amount of contrast media applied and the examination quality. Complications were graded in minor (contrast leakage, premature termination of the examination) and major (fever, urinary tract infection, bladder perforation). Fluoroscopy time and radiation parameters were compared. Examination quality was assessed based on the satisfactory acquisition of fluoroscopic images using a four-point Likert scale.
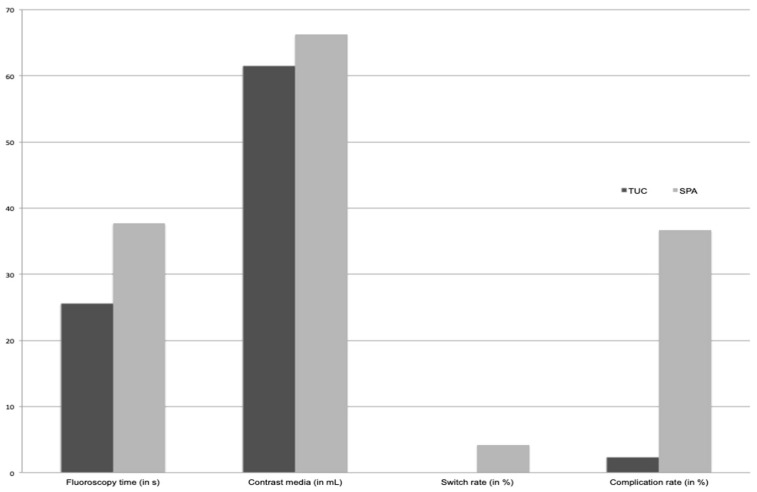
Results: In 9% of the SPA examinations a method switch to TUC was necessary. The minor complication rate was 1.9% for TUC and 35.7% for SPA (p < 0.001). The major complication rate was 0.9% for TUC and 2% for SPA (p > 0.05). Mean fluoroscopy time and radiation dose were significantly lower in TUC (TUC, 26 ± 19 s, 0.6 ± 1.2 µGy·m2; SPA, 38 ± 33 s, 1.7 ± 2.9 µGy·m2; p = 0.01/0.001). There was no significant difference regarding the amount of contrast media applied (TUC, 62 ± 40 mL; SPA, 66 ± 41 mL; p > 0.05) and the examination quality with full diagnostic quality achieved in 88% of TUC and 89% of SPA examinations (p > 0.05).
Conclusions: As TUC provides significantly lower radiation exposure and less periprocedural complications, it should be the primary bladder access route for VCUG in pediatric male patients.
Keywords: pediatric urology; radiation dose; suprapubic puncture; transurethral catheterization; vesicoureteral reflux; voiding cystourethrography.
Conflict of interest statement
The authors declare that they have no conflicts of interest. All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
