

NPEPPS Is a Druggable Driver of Platinum Resistance
- PMID: 38535994
- PMCID: PMC11094426
- DOI: 10.1158/0008-5472.CAN-23-1976
NPEPPS Is a Druggable Driver of Platinum Resistance
Abstract
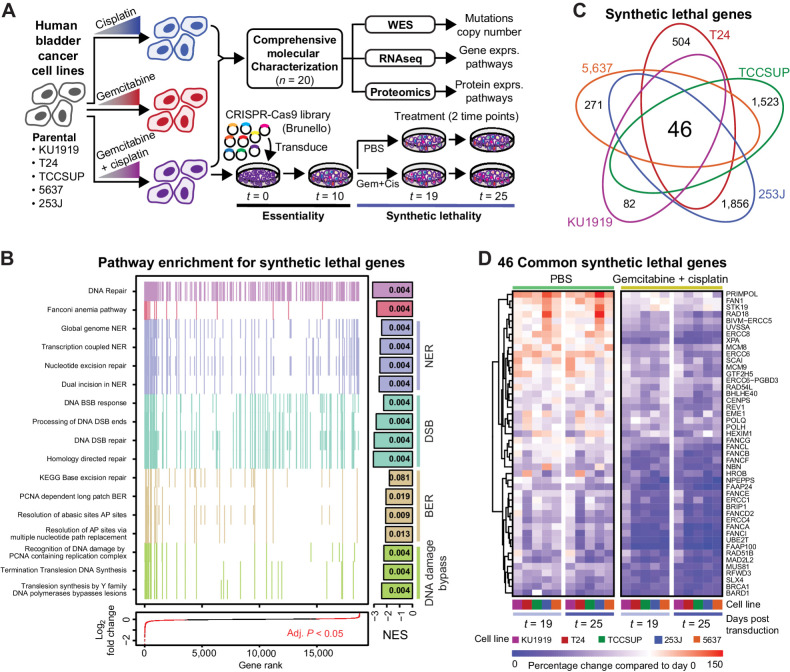
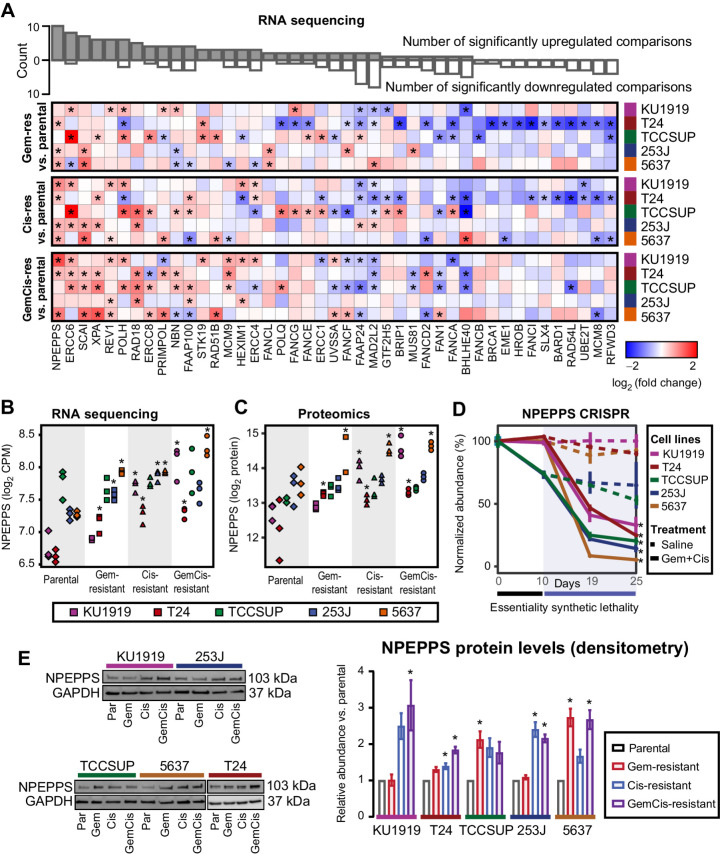
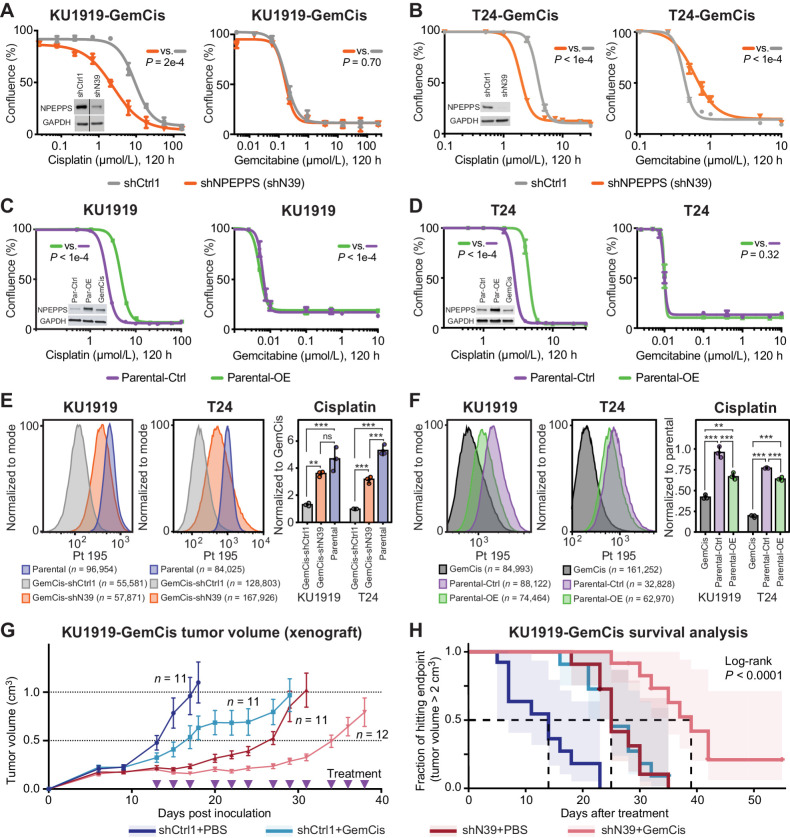
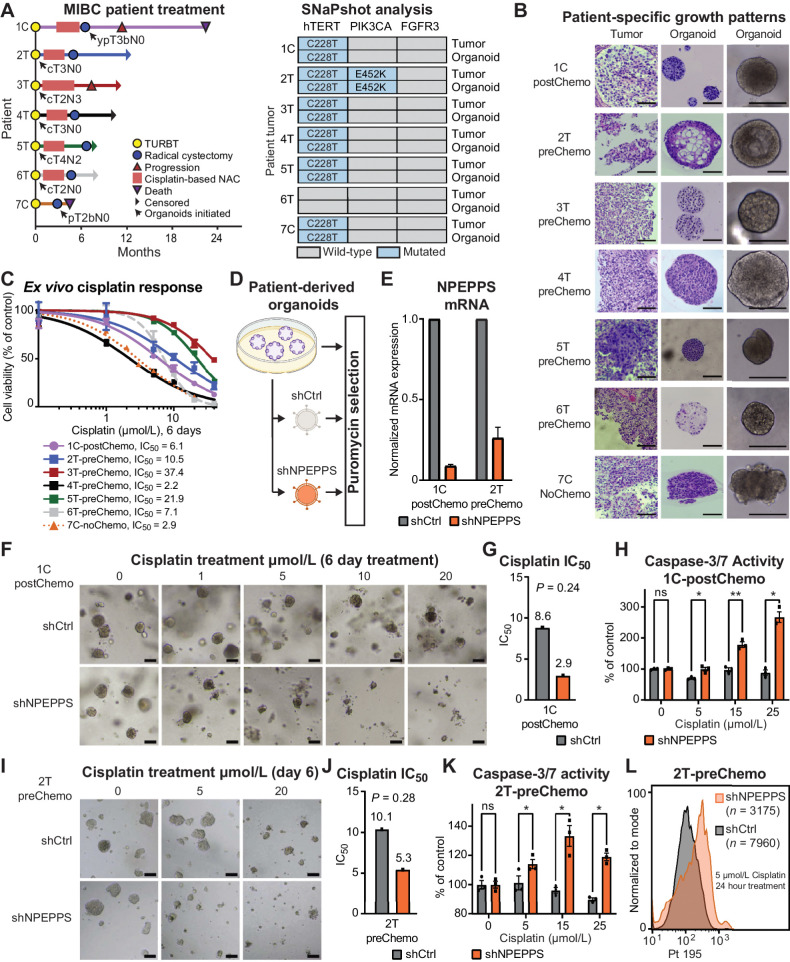
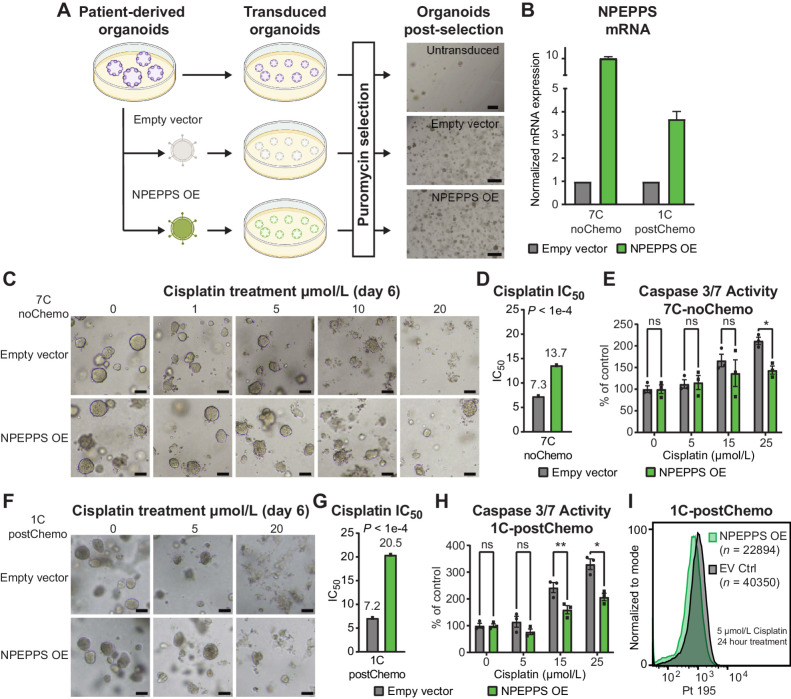
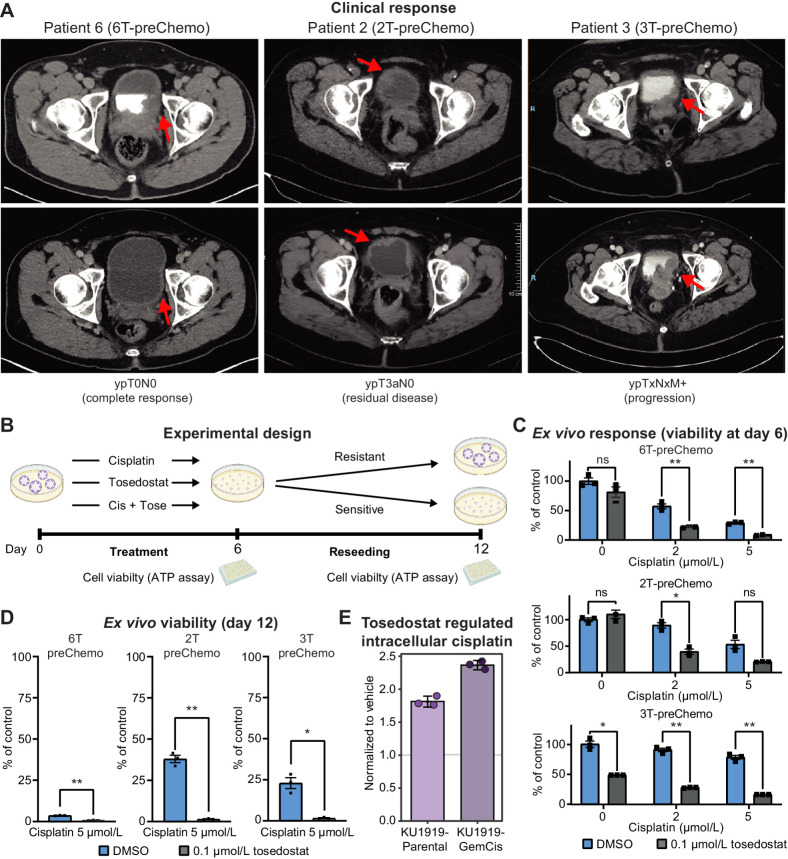
There is an unmet need to improve the efficacy of platinum-based cancer chemotherapy, which is used in primary and metastatic settings in many cancer types. In bladder cancer, platinum-based chemotherapy leads to better outcomes in a subset of patients when used in the neoadjuvant setting or in combination with immunotherapy for advanced disease. Despite such promising results, extending the benefits of platinum drugs to a greater number of patients is highly desirable. Using the multiomic assessment of cisplatin-responsive and -resistant human bladder cancer cell lines and whole-genome CRISPR screens, we identified puromycin-sensitive aminopeptidase (NPEPPS) as a driver of cisplatin resistance. NPEPPS depletion sensitized resistant bladder cancer cells to cisplatin in vitro and in vivo. Conversely, overexpression of NPEPPS in sensitive cells increased cisplatin resistance. NPEPPS affected treatment response by regulating intracellular cisplatin concentrations. Patient-derived organoids (PDO) generated from bladder cancer samples before and after cisplatin-based treatment, and from patients who did not receive cisplatin, were evaluated for sensitivity to cisplatin, which was concordant with clinical response. In the PDOs, depletion or pharmacologic inhibition of NPEPPS increased cisplatin sensitivity, while NPEPPS overexpression conferred resistance. Our data present NPEPPS as a druggable driver of cisplatin resistance by regulating intracellular cisplatin concentrations.
Significance: Targeting NPEPPS, which induces cisplatin resistance by controlling intracellular drug concentrations, is a potential strategy to improve patient responses to platinum-based therapies and lower treatment-associated toxicities.
©2024 The Authors; Published by the American Association for Cancer Research.
Figures
References
-
- Dilruba S, Kalayda GV. Platinum-based drugs: past, present and future. Cancer Chemother Pharmacol 2016;77:1103–24. - PubMed
-
- Rottenberg S, Disler C, Perego P. The rediscovery of platinum-based cancer therapy. Nat Rev Cancer 2021;21:37–50. - PubMed
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–49. - PubMed
MeSH terms
Substances
Grants and funding
- GM007635/National Institute of General Medical Sciences (NIGMS)
- CA268055/National Cancer Institute (NCI)
- GM008497/National Institute of General Medical Sciences (NIGMS)
- T32 GM008497/GM/NIGMS NIH HHS/United States
- 111296/Erasmus Medisch Centrum (EMC)
- CA180175/National Cancer Institute (NCI)
- Finnish Cancer Institute (Suomen syöpälaitos)
- CA046934/National Cancer Institute (NCI)
- P30 CA046934/CA/NCI NIH HHS/United States
- Anschutz Family Foundation
- 107088/Erasmus Medisch Centrum (EMC)
- T32 GM007635/GM/NIGMS NIH HHS/United States
- R01 CA180175/CA/NCI NIH HHS/United States
- R01 CA268055/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
