

Enhancing a deep learning model for pulmonary nodule malignancy risk estimation in chest CT with uncertainty estimation
- PMID: 38536463
- PMCID: PMC11399205
- DOI: 10.1007/s00330-024-10714-7
Enhancing a deep learning model for pulmonary nodule malignancy risk estimation in chest CT with uncertainty estimation
Abstract
Objective: To investigate the effect of uncertainty estimation on the performance of a Deep Learning (DL) algorithm for estimating malignancy risk of pulmonary nodules.
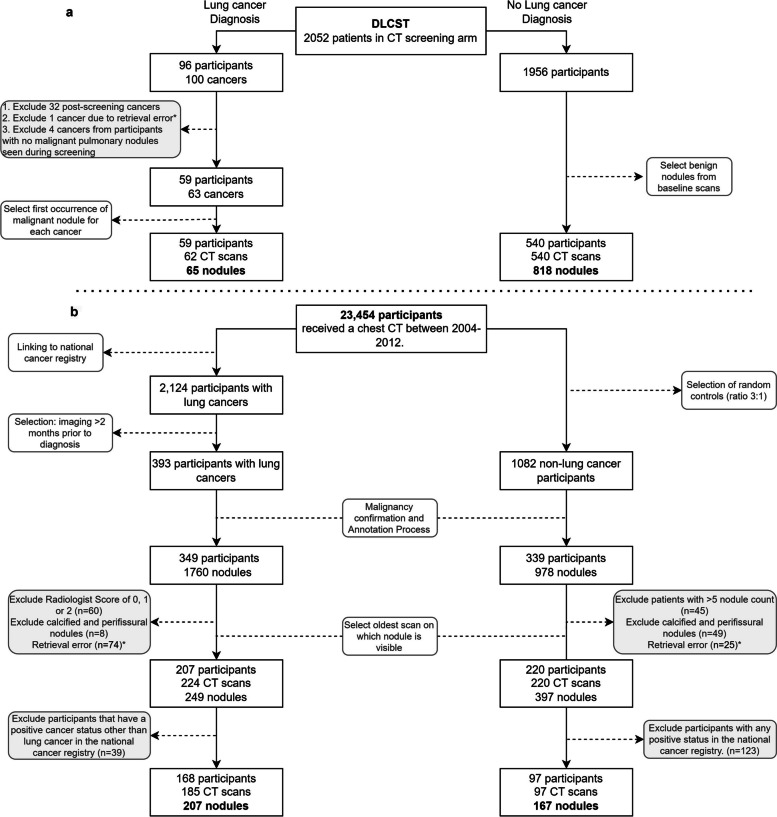
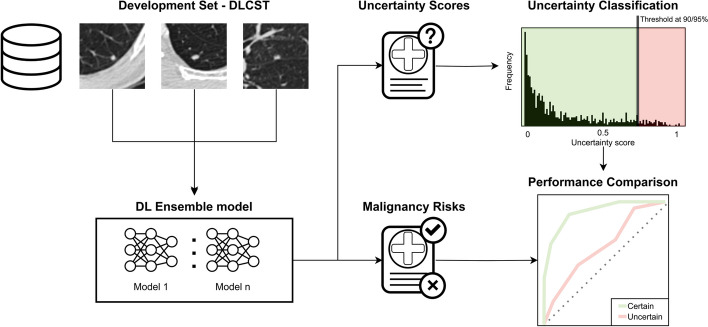
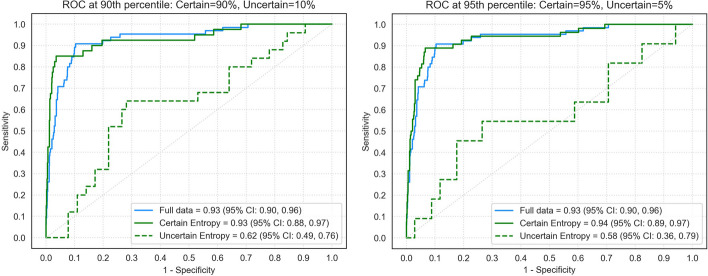
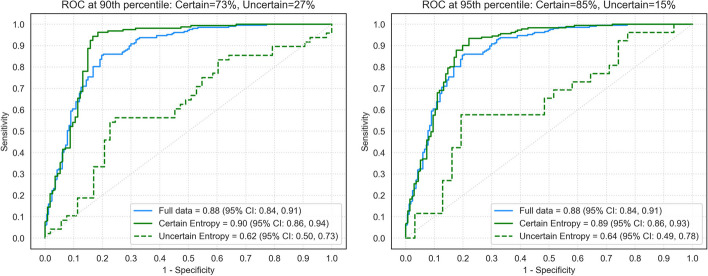
Methods and materials: In this retrospective study, we integrated an uncertainty estimation method into a previously developed DL algorithm for nodule malignancy risk estimation. Uncertainty thresholds were developed using CT data from the Danish Lung Cancer Screening Trial (DLCST), containing 883 nodules (65 malignant) collected between 2004 and 2010. We used thresholds on the 90th and 95th percentiles of the uncertainty score distribution to categorize nodules into certain and uncertain groups. External validation was performed on clinical CT data from a tertiary academic center containing 374 nodules (207 malignant) collected between 2004 and 2012. DL performance was measured using area under the ROC curve (AUC) for the full set of nodules, for the certain cases and for the uncertain cases. Additionally, nodule characteristics were compared to identify trends for inducing uncertainty.
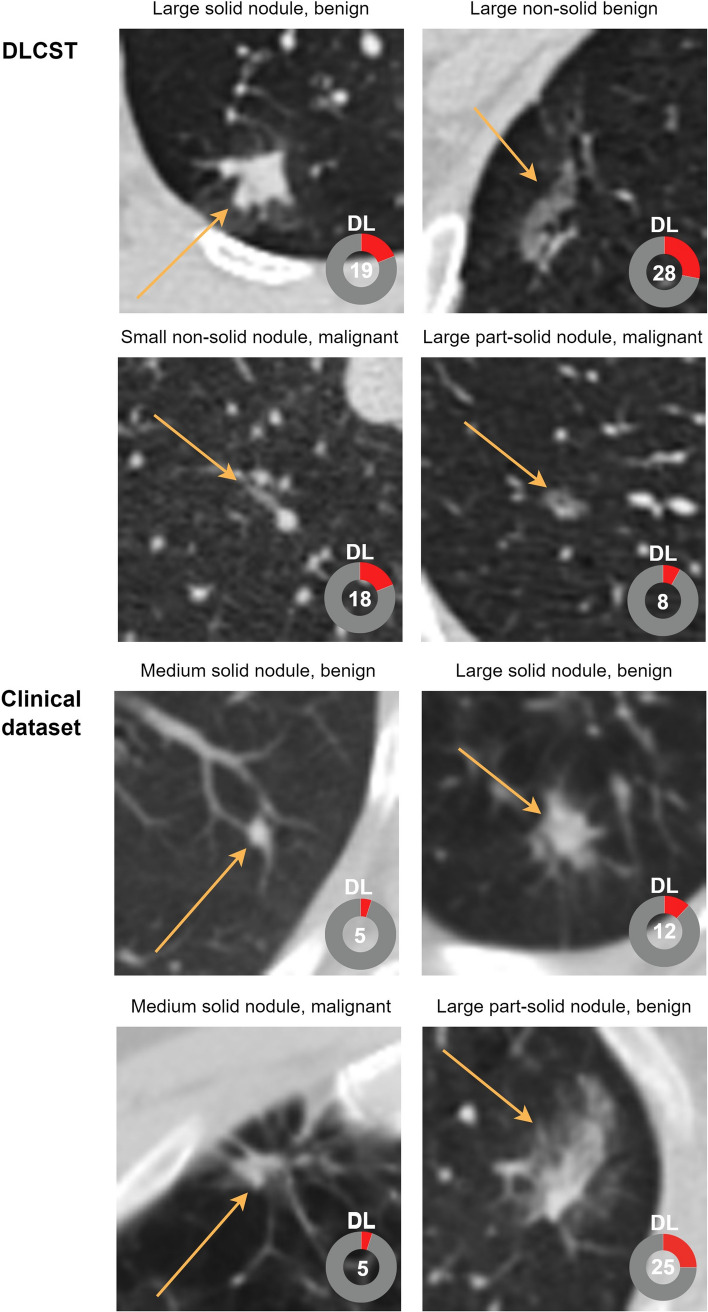
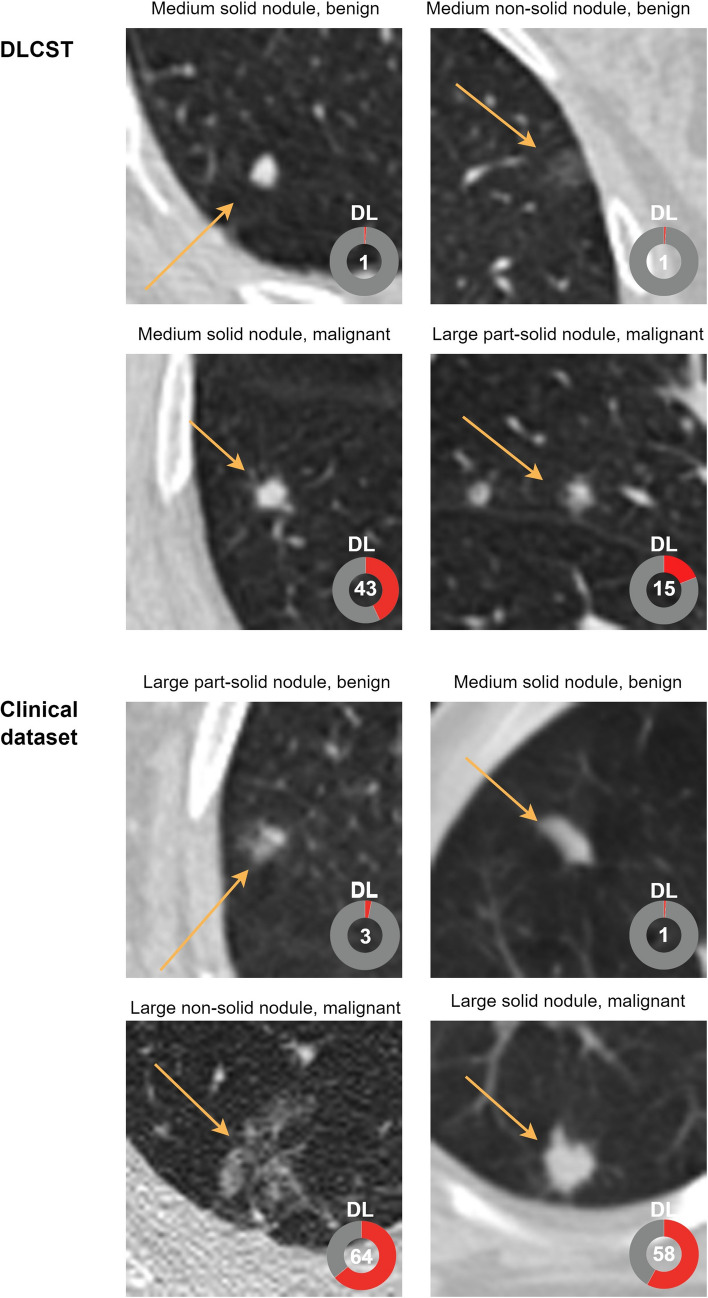
Results: The DL algorithm performed significantly worse in the uncertain group compared to the certain group of DLCST (AUC 0.62 (95% CI: 0.49, 0.76) vs 0.93 (95% CI: 0.88, 0.97); p < .001) and the clinical dataset (AUC 0.62 (95% CI: 0.50, 0.73) vs 0.90 (95% CI: 0.86, 0.94); p < .001). The uncertain group included larger benign nodules as well as more part-solid and non-solid nodules than the certain group.
Conclusion: The integrated uncertainty estimation showed excellent performance for identifying uncertain cases in which the DL-based nodule malignancy risk estimation algorithm had significantly worse performance.
Clinical relevance statement: Deep Learning algorithms often lack the ability to gauge and communicate uncertainty. For safe clinical implementation, uncertainty estimation is of pivotal importance to identify cases where the deep learning algorithm harbors doubt in its prediction.
Key points: • Deep learning (DL) algorithms often lack uncertainty estimation, which potentially reduce the risk of errors and improve safety during clinical adoption of the DL algorithm. • Uncertainty estimation identifies pulmonary nodules in which the discriminative performance of the DL algorithm is significantly worse. • Uncertainty estimation can further enhance the benefits of the DL algorithm and improve its safety and trustworthiness.
Keywords: Deep learning; Multiple pulmonary nodules; Tomography (X-ray computed); Uncertainty.
© 2024. The Author(s).
Conflict of interest statement
The authors declare the following competing interests:
MP receives grants from Canon Medical Systems, Siemens Healthineers; royalties from Mevis Medical Solutions; and payment for lectures from Canon Medical Systems and Siemens Healthineers. The host institution of MP is a minority shareholder in Thirona. He reports no other relationships that are related to the subject matter of the article.
The host institution of CJ receives research grants and royalties from MeVis Medical Solutions, Bremen, Germany, and payment for lectures from Canon Medical Systems. CJ is a collaborator in a public-private research project where Radboudumc collaborates with Philips Medical Systems (Best, the Netherlands). CJ is a member of the Scientific Editorial Board for
The host institution of HH receives grants from Siemens Healthineers. He reports no other relationships that are related to the subject matter of the article.
RV is supported by an institutional research grant from Siemens Healthineers.
Figures
Similar articles
-
Deep Learning for Malignancy Risk Estimation of Pulmonary Nodules Detected at Low-Dose Screening CT.Radiology. 2021 Aug;300(2):438-447. doi: 10.1148/radiol.2021204433. Epub 2021 May 18. Radiology. 2021. PMID: 34003056
-
Deep learning for malignancy risk estimation of incidental sub-centimeter pulmonary nodules on CT images.Eur Radiol. 2024 Jul;34(7):4218-4229. doi: 10.1007/s00330-023-10518-1. Epub 2023 Dec 20. Eur Radiol. 2024. PMID: 38114849
-
Prior CT Improves Deep Learning for Malignancy Risk Estimation of Screening-detected Pulmonary Nodules.Radiology. 2023 Aug;308(2):e223308. doi: 10.1148/radiol.223308. Radiology. 2023. PMID: 37526548
-
Deep Learning Models for Predicting Malignancy Risk in CT-Detected Pulmonary Nodules: A Systematic Review and Meta-analysis.Lung. 2024 Oct;202(5):625-636. doi: 10.1007/s00408-024-00706-1. Epub 2024 May 23. Lung. 2024. PMID: 38782779 Free PMC article.
-
Evaluating the Patient With a Pulmonary Nodule: A Review.JAMA. 2022 Jan 18;327(3):264-273. doi: 10.1001/jama.2021.24287. JAMA. 2022. PMID: 35040882 Review.
Cited by
-
Diagnostic accuracy of deep learning for the invasiveness assessment of ground-glass nodules with fine segmentation: a systematic review and meta-analysis.Quant Imaging Med Surg. 2025 Apr 1;15(4):2722-2738. doi: 10.21037/qims-24-1839. Epub 2025 Mar 28. Quant Imaging Med Surg. 2025. PMID: 40235789 Free PMC article.
-
Artificial Intelligence interpretation of chest radiographs in intensive care. Ready for prime time?Intensive Care Med. 2025 Jan;51(1):154-156. doi: 10.1007/s00134-024-07725-9. Epub 2024 Nov 20. Intensive Care Med. 2025. PMID: 39565379 No abstract available.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
