

Automated graded prognostic assessment for patients with hepatocellular carcinoma using machine learning
- PMID: 38536464
- PMCID: PMC11399284
- DOI: 10.1007/s00330-024-10624-8
Automated graded prognostic assessment for patients with hepatocellular carcinoma using machine learning
Abstract
Background: Accurate mortality risk quantification is crucial for the management of hepatocellular carcinoma (HCC); however, most scoring systems are subjective.
Purpose: To develop and independently validate a machine learning mortality risk quantification method for HCC patients using standard-of-care clinical data and liver radiomics on baseline magnetic resonance imaging (MRI).
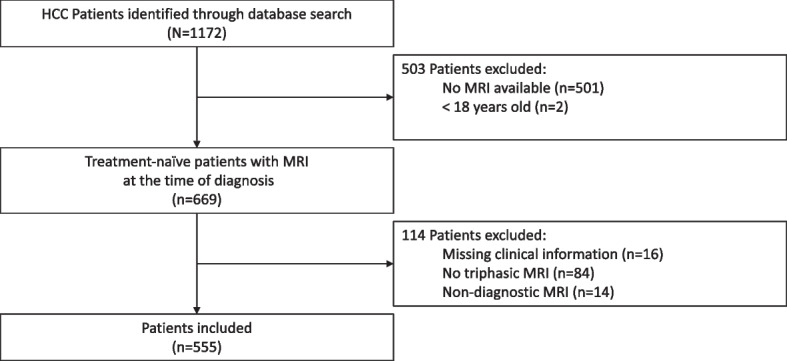
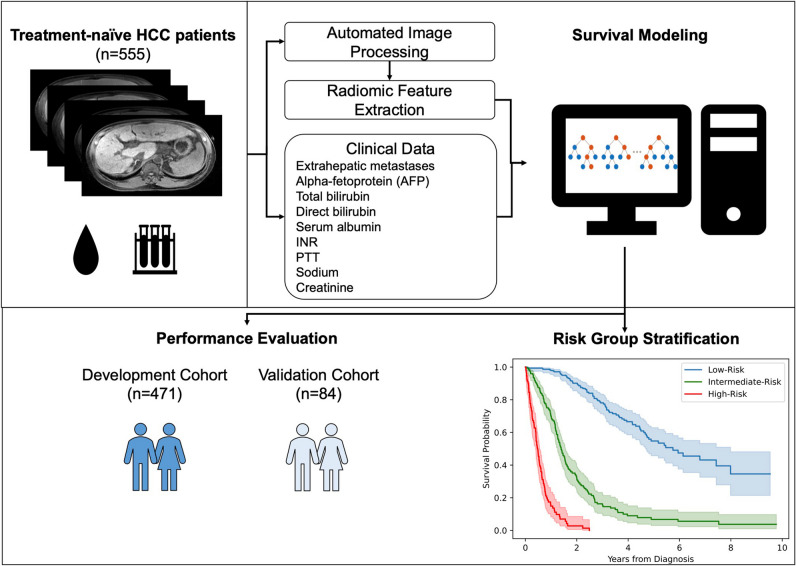
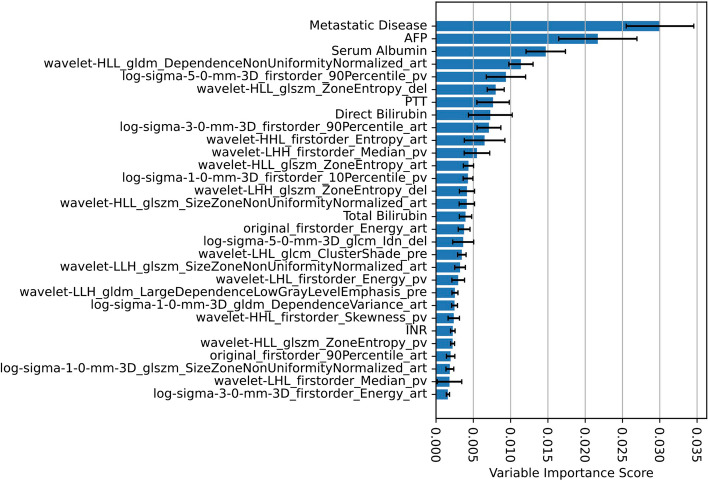
Methods: This retrospective study included all patients with multiphasic contrast-enhanced MRI at the time of diagnosis treated at our institution. Patients were censored at their last date of follow-up, end-of-observation, or liver transplantation date. The data were randomly sampled into independent cohorts, with 85% for development and 15% for independent validation. An automated liver segmentation framework was adopted for radiomic feature extraction. A random survival forest combined clinical and radiomic variables to predict overall survival (OS), and performance was evaluated using Harrell's C-index.
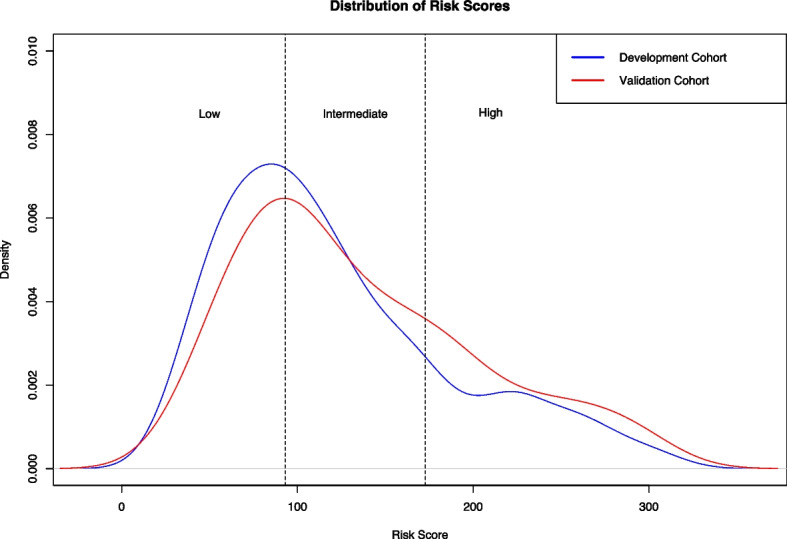
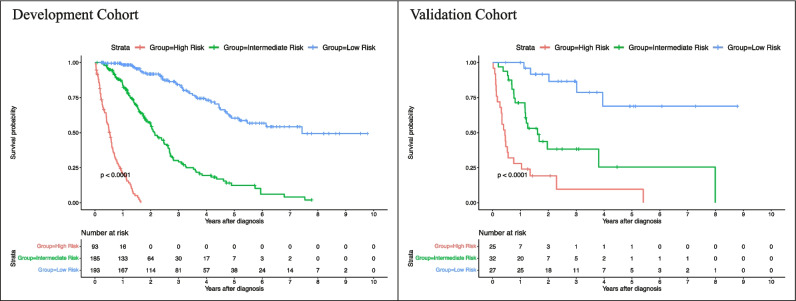
Results: A total of 555 treatment-naïve HCC patients (mean age, 63.8 years ± 8.9 [standard deviation]; 118 females) with MRI at the time of diagnosis were included, of which 287 (51.7%) died after a median time of 14.40 (interquartile range, 22.23) months, and had median followed up of 32.47 (interquartile range, 61.5) months. The developed risk prediction framework required 1.11 min on average and yielded C-indices of 0.8503 and 0.8234 in the development and independent validation cohorts, respectively, outperforming conventional clinical staging systems. Predicted risk scores were significantly associated with OS (p < .00001 in both cohorts).
Conclusions: Machine learning reliably, rapidly, and reproducibly predicts mortality risk in patients with hepatocellular carcinoma from data routinely acquired in clinical practice.
Clinical relevance statement: Precision mortality risk prediction using routinely available standard-of-care clinical data and automated MRI radiomic features could enable personalized follow-up strategies, guide management decisions, and improve clinical workflow efficiency in tumor boards.
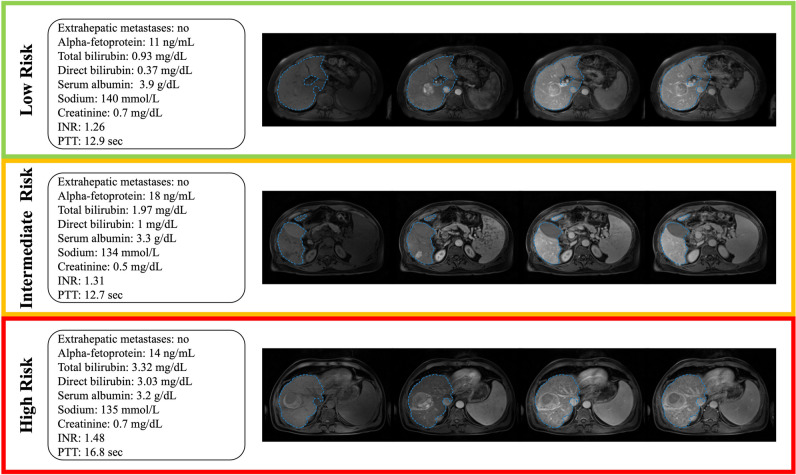
Key points: • Machine learning enables hepatocellular carcinoma mortality risk prediction using standard-of-care clinical data and automated radiomic features from multiphasic contrast-enhanced MRI. • Automated mortality risk prediction achieved state-of-the-art performances for mortality risk quantification and outperformed conventional clinical staging systems. • Patients were stratified into low, intermediate, and high-risk groups with significantly different survival times, generalizable to an independent evaluation cohort.
Keywords: Hepatocellular carcinoma; Machine learning; Magnetic resonance imaging; Medical image processing; Risk assessment.
© 2024. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
