

Delirium and incident dementia in hospital patients in New South Wales, Australia: retrospective cohort study
- PMID: 38537951
- PMCID: PMC10966895
- DOI: 10.1136/bmj-2023-077634
Delirium and incident dementia in hospital patients in New South Wales, Australia: retrospective cohort study
Abstract
Objectives: To determine the strength and nature of the association between delirium and incident dementia in a population of older adult patients without dementia at baseline.
Design: Retrospective cohort study using large scale hospital administrative data.
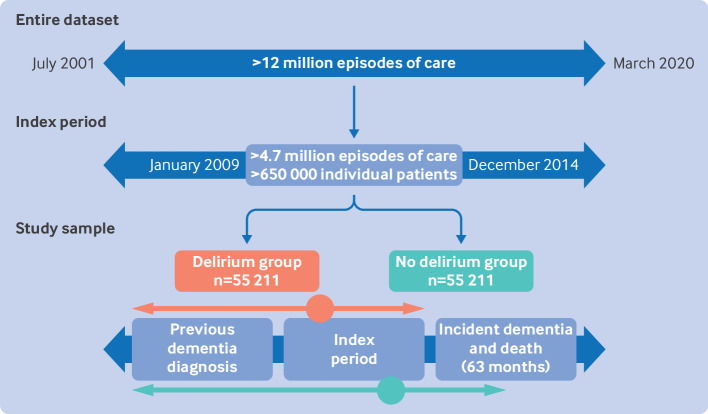
Setting: Public and private hospitals in New South Wales, Australia between July 2001 and March 2020.
Participants: Data were extracted for 650 590 hospital patients aged ≥65 years. Diagnoses of dementia and delirium were identified from ICD-10 (international classification of diseases, 10th revision) codes. Patients with dementia at baseline were excluded. Delirium-no delirium pairs were identified by matching personal and clinical characteristics, and were followed for more than five years.
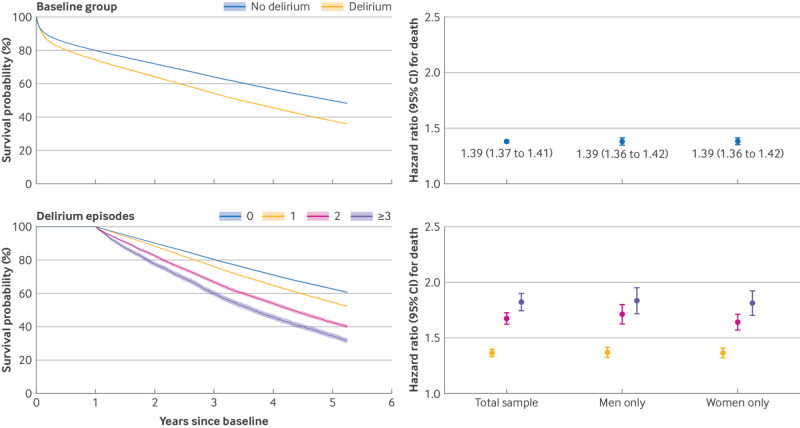
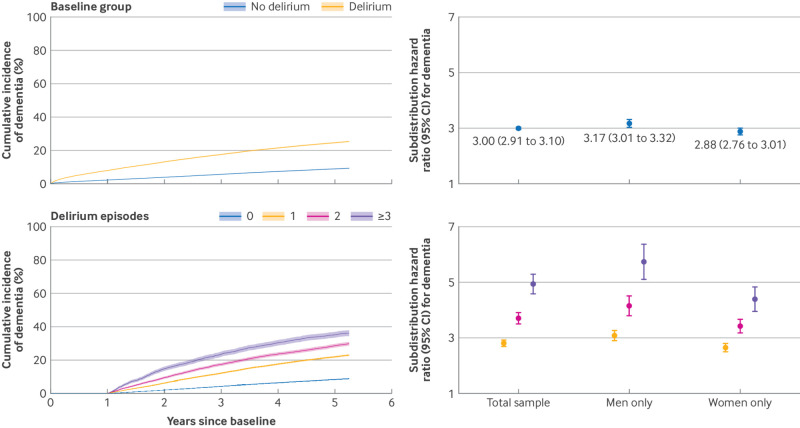
Main outcome measures: Cox proportional hazards models and Fine-Gray hazard models were used to estimate the associations of delirium with death and incident dementia, respectively. Delirium-outcome dose-response associations were quantified, all analyses were performed in men and women separately, and sensitivity analyses were conducted.
Results: The study included 55 211 matched pairs (48% men, mean age 83.4 years, standard deviation 6.5 years). Collectively, 58% (n=63 929) of patients died and 17% (n=19 117) had a newly reported dementia diagnosis during 5.25 years of follow-up. Patients with delirium had 39% higher risk of death (hazard ratio 1.39, 95% confidence interval 1.37 to 1.41) and three times higher risk of incident dementia (subdistribution hazard ratio 3.00, 95% confidence interval 2.91 to 3.10) than patients without delirium. The association with dementia was stronger in men (P=0.004). Each additional episode of delirium was associated with a 20% increased risk of dementia (subdistribution hazard ratio 1.20, 95% confidence interval 1.18 to 1.23).
Conclusions: The study findings suggest delirium was a strong risk factor for death and incident dementia among older adult patients. The data support a causal interpretation of the association between delirium and dementia. The clinical implications of delirium as a potentially modifiable risk factor for dementia are substantial.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at https://www.icmje.org/disclosure-of-interest/ and declare: support from National Health and Medical Research Council: Partnership Centre for Health System Sustainability for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical