

Derivation and external validation of a simple risk score for predicting severe acute kidney injury after intravenous cisplatin: cohort study
- PMID: 38538012
- PMCID: PMC10964715
- DOI: 10.1136/bmj-2023-077169
Derivation and external validation of a simple risk score for predicting severe acute kidney injury after intravenous cisplatin: cohort study
Erratum in
-
Derivation and external validation of a simple risk score for predicting severe acute kidney injury after intravenous cisplatin: cohort study.BMJ. 2024 Jun 20;385:q1207. doi: 10.1136/bmj.q1207. BMJ. 2024. PMID: 38901848 Free PMC article. No abstract available.
Abstract
Objective: To develop and externally validate a prediction model for severe cisplatin associated acute kidney injury (CP-AKI).
Design: Multicenter cohort study.
Setting: Six geographically diverse major academic cancer centers across the US.
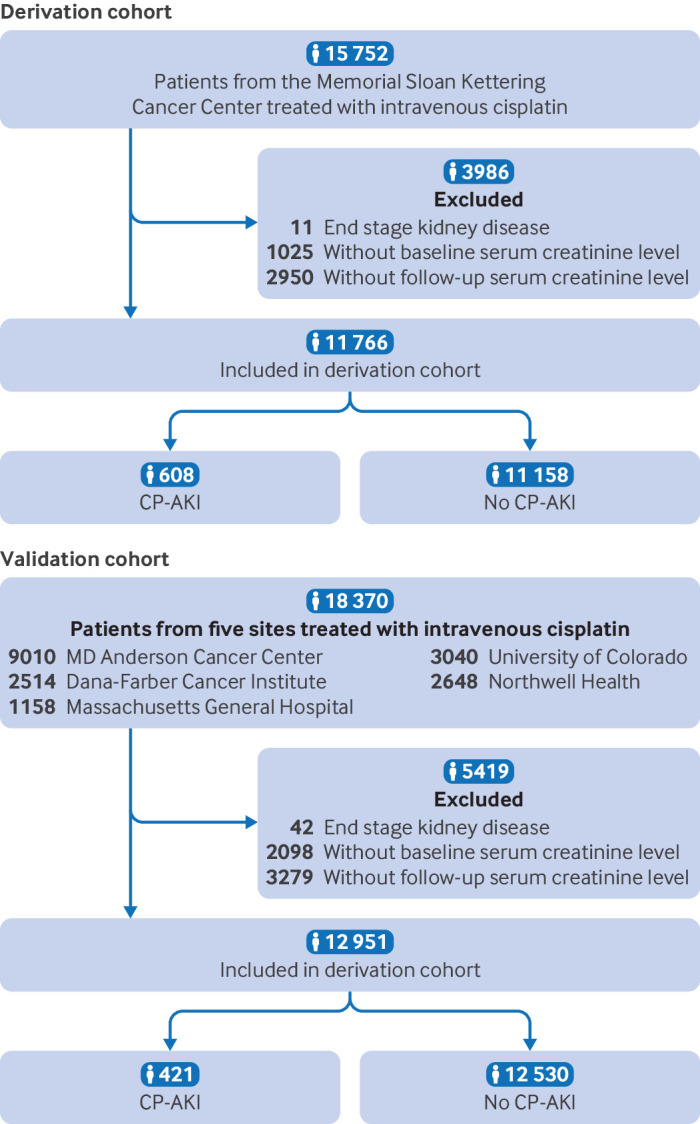
Participants: Adults (≥18 years) receiving their first dose of intravenous cisplatin, 2006-22.
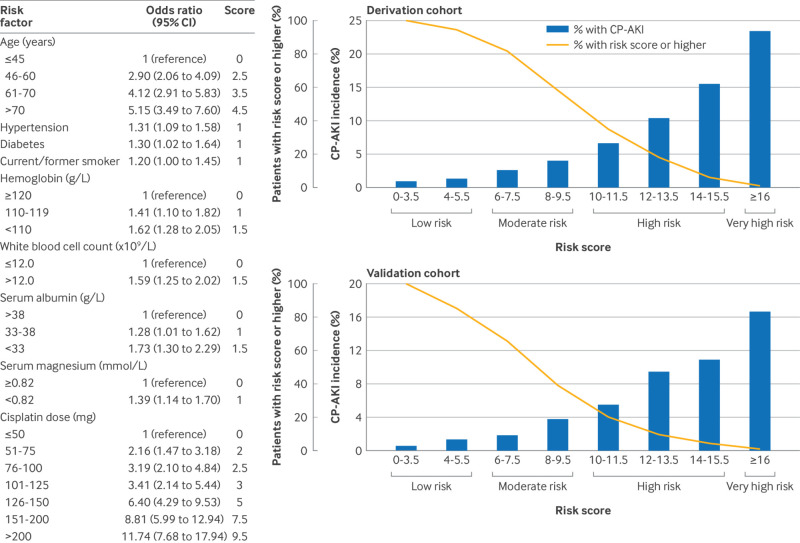
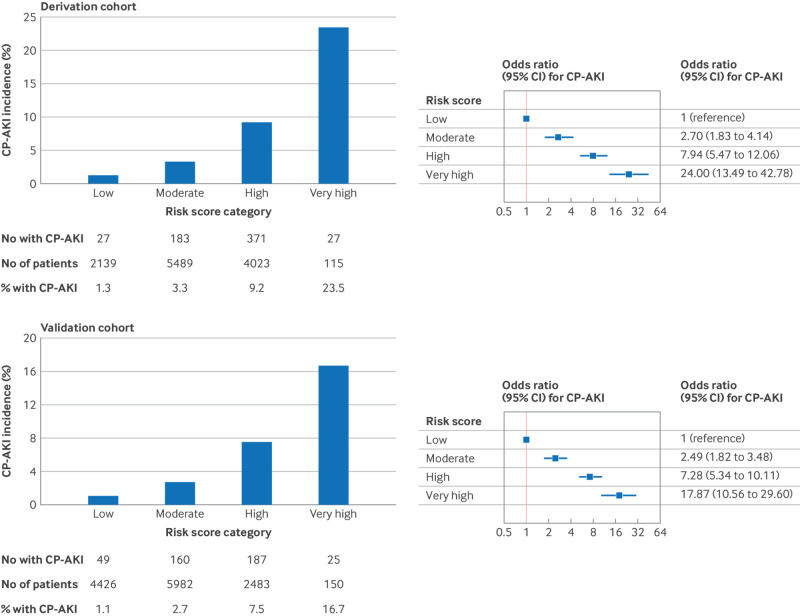
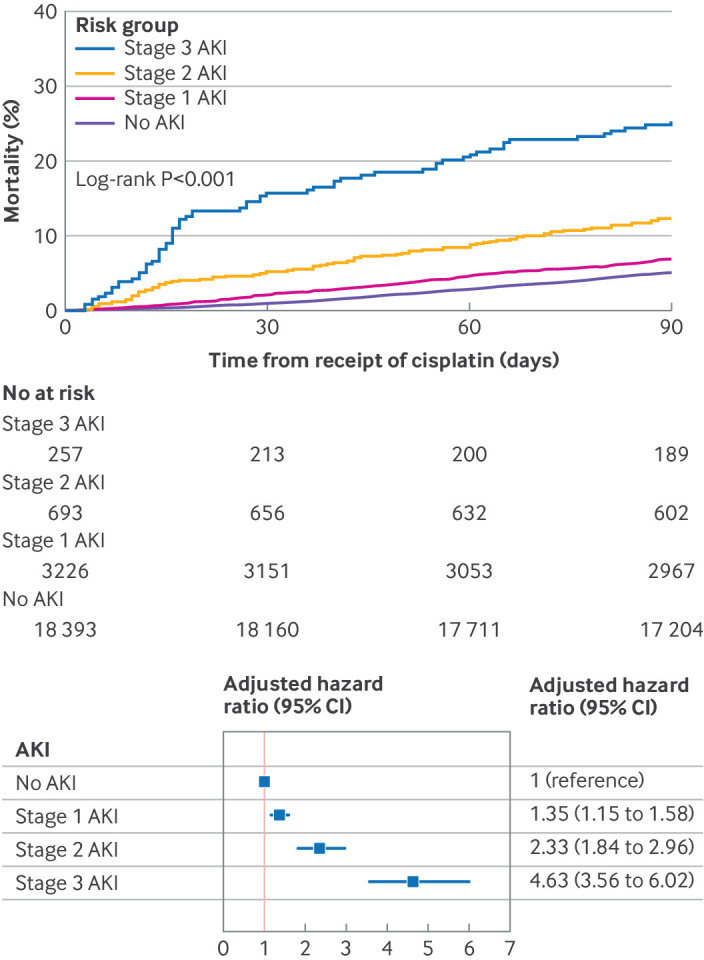
Main outcome measures: The primary outcome was CP-AKI, defined as a twofold or greater increase in serum creatinine or kidney replacement therapy within 14 days of a first dose of intravenous cisplatin. Independent predictors of CP-AKI were identified using a multivariable logistic regression model, which was developed in a derivation cohort and tested in an external validation cohort. For the primary model, continuous variables were examined using restricted cubic splines. A simple risk model was also generated by converting the odds ratios from the primary model into risk points. Finally, a multivariable Cox model was used to examine the association between severity of CP-AKI and 90 day survival.
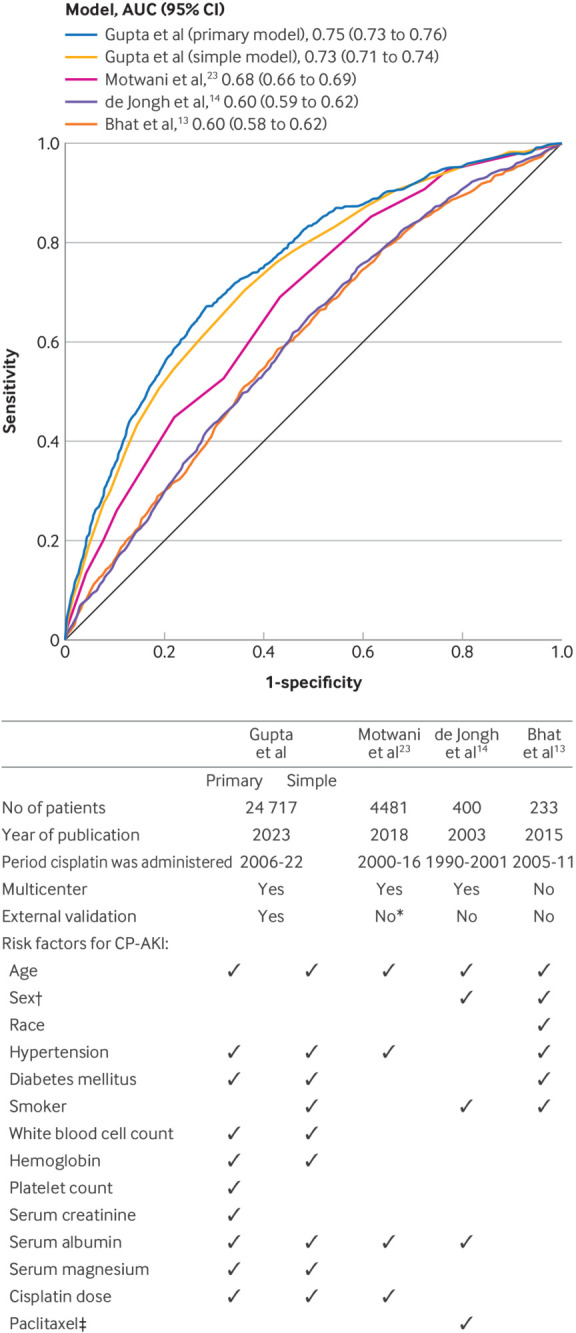
Results: A total of 24 717 adults were included, with 11 766 in the derivation cohort (median age 59 (interquartile range (IQR) 50-67)) and 12 951 in the validation cohort (median age 60 (IQR 50-67)). The incidence of CP-AKI was 5.2% (608/11 766) in the derivation cohort and 3.3% (421/12 951) in the validation cohort. Each of the following factors were independently associated with CP-AKI in the derivation cohort: age, hypertension, diabetes mellitus, serum creatinine level, hemoglobin level, white blood cell count, platelet count, serum albumin level, serum magnesium level, and cisplatin dose. A simple risk score consisting of nine covariates was shown to predict a higher risk of CP-AKI in a monotonic fashion in both the derivation cohort and the validation cohort. Compared with patients in the lowest risk category, those in the highest risk category showed a 24.00-fold (95% confidence interval (CI) 13.49-fold to 42.78-fold) higher odds of CP-AKI in the derivation cohort and a 17.87-fold (10.56-fold to 29.60-fold) higher odds in the validation cohort. The primary model had a C statistic of 0.75 and showed better discrimination for CP-AKI than previously published models, the C statistics for which ranged from 0.60 to 0.68 (DeLong P<0.001 for each comparison). Greater severity of CP-AKI was monotonically associated with shorter 90 day survival (adjusted hazard ratio 4.63 (95% CI 3.56 to 6.02) for stage 3 CP-AKI versus no CP-AKI).
Conclusion: This study found that a simple risk score based on readily available variables from patients receiving intravenous cisplatin could predict the risk of severe CP-AKI, the occurrence of which is strongly associated with death.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work. Outside of the submitted work, SG reports research support from the National Institutes of Health (NIH), National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) K23DK125672. She also reports research funding from BTG International, GE HealthCare, and AstraZeneca outside the submitted work. She is a member of GlaxoSmithKline’s (GSK) Global Anemia Council, a consultant for Secretome and Proletariat Therapeutics, and founder and president emeritus of the American Society of Onconephrology (unpaid). IG is supported by a Memorial Sloan Kettering Cancer Center support grant/core grant (P30CA008748). JSH serves on chronic kidney disease scientific advisory boards for Boehringer Ingelheim and the Kinetix Group. MES reports research support from the NIH, NIDDK R01DK140839. She also reports research funding from Gilead, Abbvie, Merck, Roche/Genetech, Novartis, Cabaletta, EMD-Serono, Otsuka, and Angion outside of the submitted work. She has served on a scientific advisory board for Travere, Novartis, Vera, Calliditas, and Mallinckrodt, is a data monitoring committee member for Alpine Immunosciences, and consults for Resonance. KDJ is a cofounder of the American Society of Onconephrology and reports consultancy agreements with Secretome, George Clinicals, PMV pharmaceuticals, Otsuka, and Calliditas, reports honorariums from the American Society of Nephrology, Lexicomp, and UpToDate.com; and reports serving as editor in chief of ASN Kidney News, and section editor for onconephrology for Nephrology Dialysis Transplantation. WX is supported by Department of Defense W81XWH2210951 and reports research funding from Oncohost outside the scope of this work, advisory board fees from Exelixis and Jazz Pharmaceuticals, and continuing medical education honorariums from MedNet, Harborside Press, MJH Healthcare Holdings, and Academy for Continued Healthcare Learning. KS reports receiving consulting fees from Scholar Rock and Equinox Group, personal fees for consulting or advisory board participation from Exelexis and MedScape, research funding to the institution from Merck, and travel honorarium from Merck. KR receives fees for organizing educational initiatives from Medscape and CME outfitters and previously served on the advisory board for SAGA diagnostics. KR also receives funds for institutional research from Bristol Myers Squibb. DEL is supported by NIH grants R01HL144566, R01DK125786, and R01DK126685 and reports research support from BioPorto, BTG International, and Metro International Biotech, and has served as a consultant for Sidereal Therapeutics, Casma Therapeutics, and MexBrain.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous