

Exploratory Assessment of Galectin-1, -3, and -9 in Non-Small Cell Lung Cancer
- PMID: 38539500
- PMCID: PMC10969284
- DOI: 10.3390/cancers16061165
Exploratory Assessment of Galectin-1, -3, and -9 in Non-Small Cell Lung Cancer
Abstract
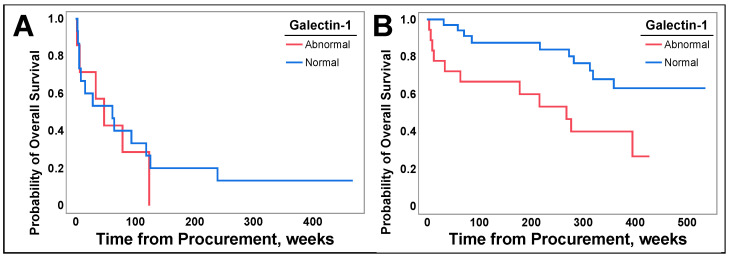
Galectins play a pivotal role in lung cancer oncogenic pathways, influencing apoptosis, angiogenesis, and tumor metastasis. Biomarkers that diagnose, prognose, and guide cancer treatment are crucial, with galectins having the biomarker potential for non-small cell lung cancer (NSCLC). Using enzyme-linked immunosorbent assay (ELISA), we assessed serum galectin-1, -3, and -9 levels in NSCLC patients. A retrospective chart review was performed to examine patient demographics, cancer stage, tumor biology, cancer treatment, and patient outcomes. Galectin levels were then compared across these factors. In this exploratory analysis, galectin-3 levels were significantly lower in patients with squamous cell lung cancer (p = 0.0019) and in patients exposed to chemotherapy (p = 0.0375). Galectin-1 levels were significantly lower in patients with previous metastasis but had no correlation with future metastasis. Abnormal galectin-1 levels were significantly correlated with decreased overall survival (OS) in NSCLC (p = 0.0357) and specifically in patients with surgically resectable NSCLC (p = 0.0112). However, abnormal galectin-1 levels were not found to correlate with decreased OS in multivariable analysis (p = 0.0513). These findings may have clinical implications as galectin-3 inhibitors are in trials for NSCLC. Additionally, they suggest that galectin-1 has potential as a prognostic marker for surgically resectable NSCLC.
Keywords: ELISA; NSCLC; galectins; metastasis; non-small cell lung cancer; overall survival; prognosis; treatment.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures







References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
