

Identifying Predictors of Initial Surgical Failure during Minimally Invasive Endoscopic Intracerebral Hemorrhage Evacuation
- PMID: 38540121
- PMCID: PMC10968629
- DOI: 10.3390/biomedicines12030508
Identifying Predictors of Initial Surgical Failure during Minimally Invasive Endoscopic Intracerebral Hemorrhage Evacuation
Abstract
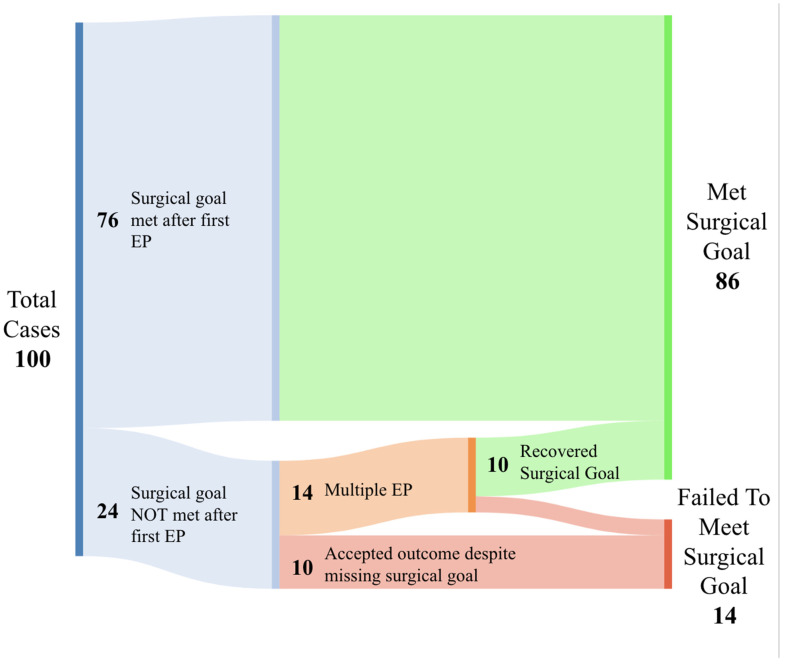
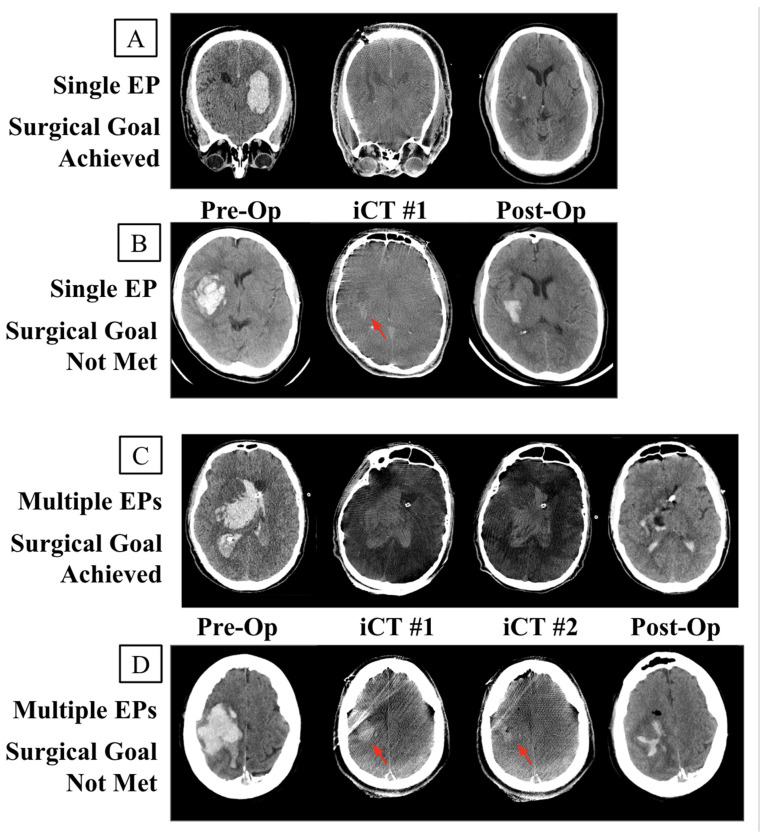
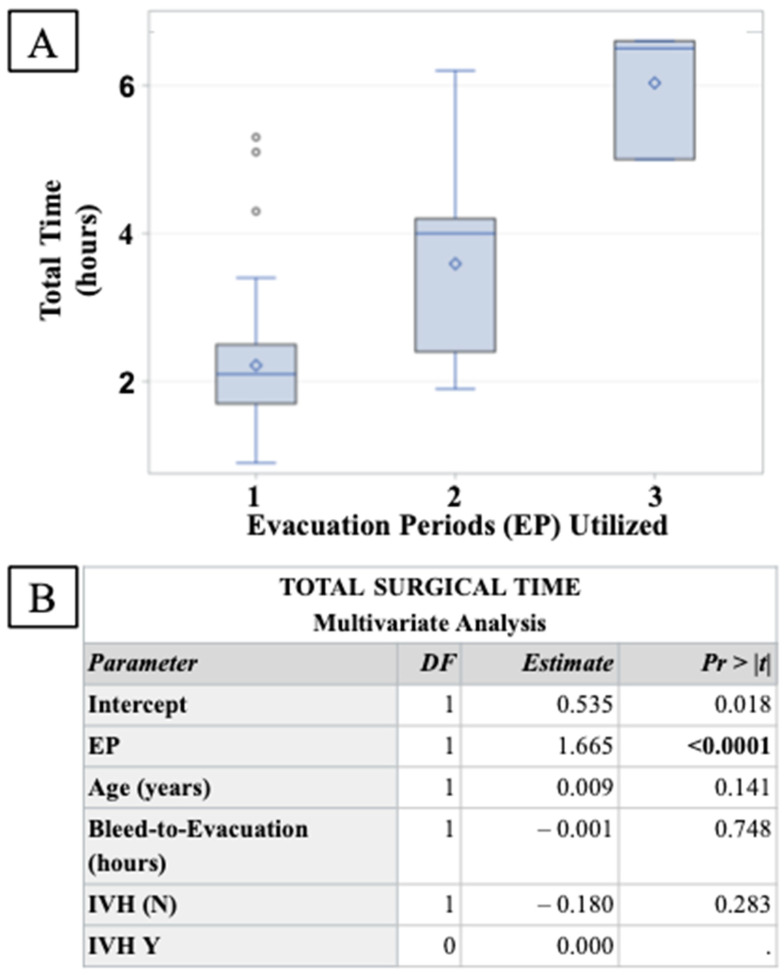
Background and Purpose: Intracerebral hemorrhage (ICH) is a common and severe disease with high rates of morbidity and mortality; however, minimally invasive surgical (MIS) hematoma evacuation represents a promising avenue for treatment. In February of 2019, the MISTIE III study found that stereotactic thrombolysis with catheter drainage did not benefit patients with supratentorial spontaneous ICH but that a clinical benefit may be present when no more than 15 mL of hematoma remains at the end of treatment. Intraoperative CT (iCT) imaging has the ability to assess whether or not this surgical goal has been met in real time, allowing for operations to add additional CT-informed 'evacuation periods' (EPs) to achieve the surgical goal. Here, we report on the frequency and predictors of initial surgical failure on at least one iCT requiring additional EPs in a large cohort of patients undergoing endoscopic minimally invasive ICH evacuation with the SCUBA technique. Methods: All patients who underwent minimally invasive endoscopic evacuation of supratentorial spontaneous ICH in a major health system between December 2015 and October 2018 were included in this study. Patient demographics, clinical and radiographic features, procedural details, and outcomes were analyzed retrospectively from a prospectively collected database. Procedures were characterized as initially successful when the first iCT demonstrated that surgical success had been achieved and initially unsuccessful when the surgical goal was not achieved, and additional EPs were performed. The surgical goal was prospectively identified in December of 2015 as leaving no more than 20% of the preoperative hematoma volume at the end of the procedure. Descriptive statistics and regression analyses were performed to identify predictors of initial failure and secondary rescue. Results: Patients (100) underwent minimally invasive endoscopic ICH evacuation in the angiography suite during the study time period. In 14 cases, the surgical goal was not met on the first iCT and multiple Eps were performed; in 10 cases the surgical goal was not met, and no additional EPs were performed. In 14 cases, the surgical goal was never achieved. When additional EPs were performed, a rescue rate of 71.4% (10/14) was seen, bringing the total percentage of cases meeting the surgical goal to 86% across the entire cohort. Cases in which the surgical goal was not achieved were significantly associated with older patients (68 years vs. 60 years; p = 0.0197) and higher rates of intraventricular hemorrhage (34.2% vs. 70.8%; p = 0.0021). Cases in which the surgical goal was rescued from initial failure had similar levels of IVH, suggesting that these additional complexities can be overcome with the use of additional iCT-informed EPs. Conclusions: Initial and ultimate surgical failure occurs in a small percentage of patients undergoing minimally invasive endoscopic ICH evacuation. The use of intraoperative imaging provides an opportunity to evaluate whether or not the surgical goal has been achieved, and to continue the procedure if the surgeon feels that more evacuation is achievable. Now that level-one evidence exists to target a surgical evacuation goal during minimally invasive ICH evacuation, intraoperative imaging, such as iCT, plays an important role in aiding the surgical team to achieve the surgical goal.
Keywords: hemorrhage; intracerebral hemorrhage; intraoperative MRI; minimally invasive surgery; stroke.
Conflict of interest statement
Christopher P. Kellner has received research grant support from Cerebrotech, Siemens, Penumbra, Minnetronix, Viz.AI, Integra, Longeviti, and Irras and has ownership in Metis Innovative and Precision Recovery.
Figures
References
-
- van Asch C.J., Luitse M.J., Rinkel G.J., van der Tweel I., Algra A., Klijn C.J. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: A systematic review and meta-analysis. Lancet Neurol. 2010;9:167–176. doi: 10.1016/S1474-4422(09)70340-0. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
