

Outcome of Different Surgical Repair Techniques for Rhegmatogenous Retinal Detachment-A Health Economic Analysis in the Split-Dalmatia County, Croatia
- PMID: 38540612
- PMCID: PMC10970497
- DOI: 10.3390/healthcare12060648
Outcome of Different Surgical Repair Techniques for Rhegmatogenous Retinal Detachment-A Health Economic Analysis in the Split-Dalmatia County, Croatia
Abstract
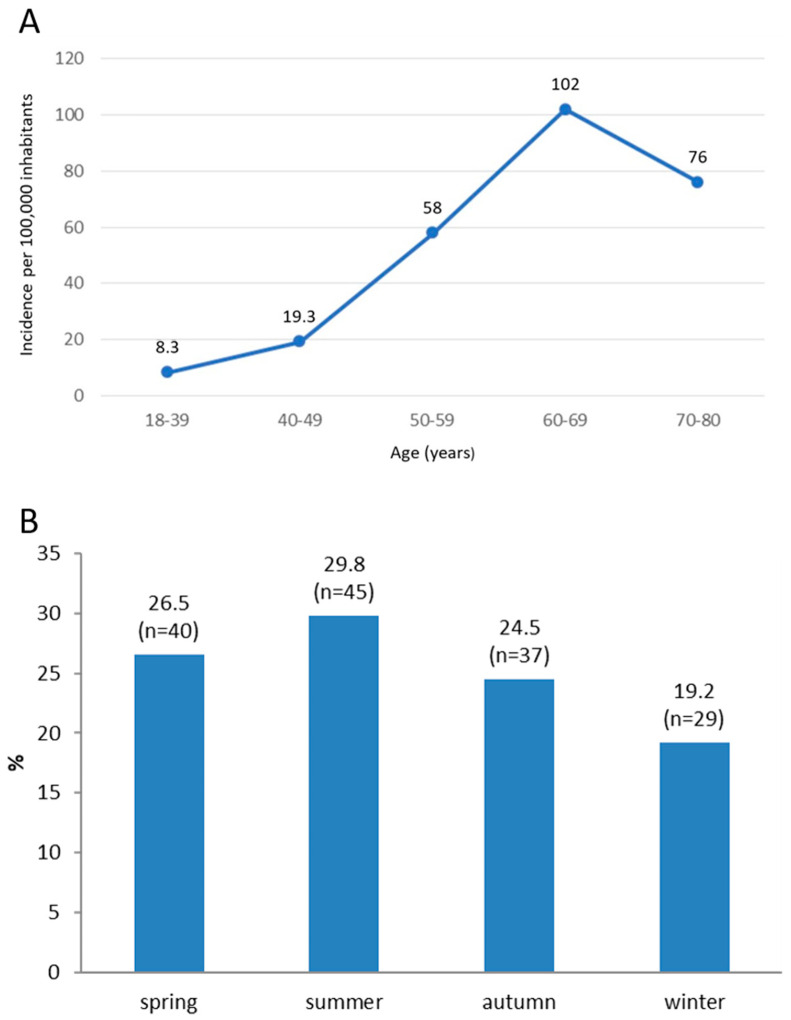
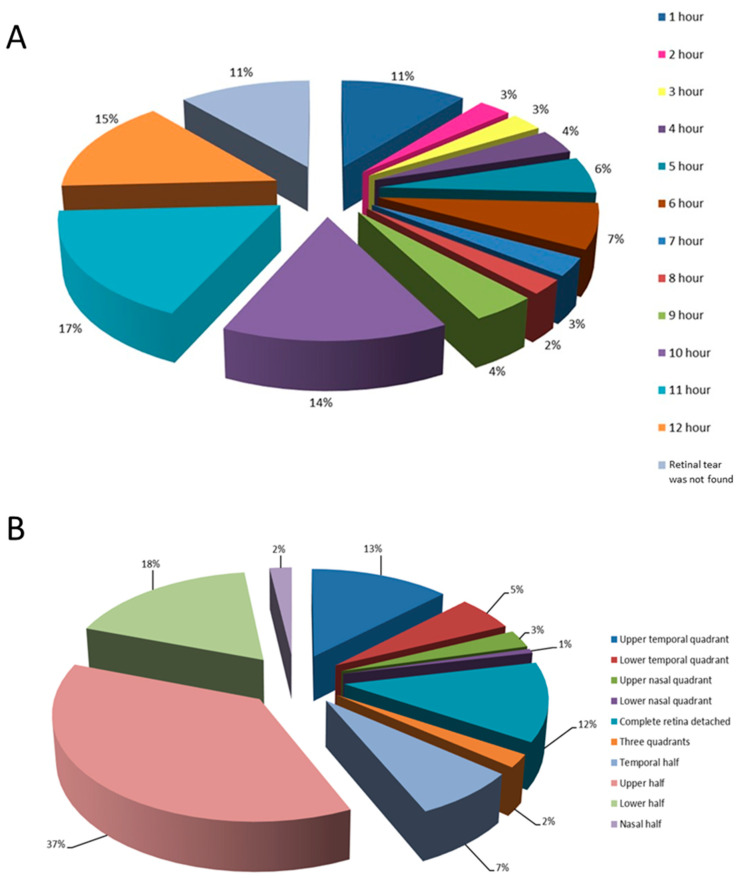
Purpose: The goal of this research is to investigate the characteristics and surgical techniques for repairing rhegmatogenous retinal detachment (RRD) and their influence on anatomical and functional success of the treatment with a special emphasis on the economic costs and outcome quality-adjusted life years (QALYs) of the procedures. Methods: This retrospective study analyzed data from 151 patients with RRD treated at the Department of Ophthalmology, Clinical Hospital Centre Split, Croatia, in a 3-year period, using one of three surgical techniques: pneumoretinopexy (PR), scleral buckling (SB) or pars plana vitrectomy (PPV), followed-up for at least 6 months. Demographic, pre- and post-operative ophthalmic exam parameters and surgical technique used were collected accordingly. Statistical analysis of the influence of the studied parameters upon anatomical and functional outcomes was performed, as well as health economic analysis on costs and derived utilities/QALYs of these surgical methods. Results: Of all patients, 130 (86%) were successfully operated on, and 21 patients (14%) required another surgical procedure. No statistically significant differences in the anatomical success between the 3 surgical techniques were found. However, the functional outcome (based on the final best corrected visual acuity (BCVA)) differed significantly. Despite improvement in the final BCVA, BCVA ≥ 0.5 was achieved in only 52 (34.4%) patients. The final BCVA showed significant association with the time elapsed from the onset of RRD to the surgical intervention, pre-operative BCVA, macular- and preoperative lens- status and type of surgery. The estimated diagnosis-related group (DRG) cost for day and inpatient surgery was based upon existing DRG cost for PPV, which for PR and SB was calculated accordingly. Based upon the success of the procedure and visual outcome, the overall calculated QALYs for PR and SB appeared to be similar, while the QALYs were lower for PPV. Conclusions: The success rate of treating RRD mostly depends on performing an early surgical procedure (especially in the case of attached macula), identification of all retina tears and, most importantly, choosing the appropriate surgical technique. Decisions on treatment for RRD should also be based upon cost-effective and QALYs-assessed procedures, especially in countries like Croatia, where limited healthcare resources exist. This study shows PR to be efficient and most cost-effective for RRD repairment in appropriate cases.
Keywords: Croatia; QALY; health economy; incidence; pars plana vitrectomy; pneumoretinopexy; retinal detachment; scleral buckling.
Conflict of interest statement
The authors declare no conflicts of interest related to the work presented here.
Figures
Similar articles
-
Pars plana vitrectomy versus scleral buckling for repairing simple rhegmatogenous retinal detachments.Cochrane Database Syst Rev. 2019 Mar 8;3(3):CD009562. doi: 10.1002/14651858.CD009562.pub2. Cochrane Database Syst Rev. 2019. PMID: 30848830 Free PMC article.
-
Primary rhegmatogenous retinal detachment - surgical methods and anatomical outcome.Acta Ophthalmol. 2017 May;95(3):247-251. doi: 10.1111/aos.13295. Epub 2016 Nov 18. Acta Ophthalmol. 2017. PMID: 27860442
-
Outcomes of Pars Plana Vitrectomy Alone versus Combined Scleral Buckling plus Pars Plana Vitrectomy for Primary Retinal Detachment.Ophthalmol Retina. 2021 Feb;5(2):169-175. doi: 10.1016/j.oret.2020.09.013. Epub 2020 Sep 25. Ophthalmol Retina. 2021. PMID: 32980532
-
Management of uncomplicated primary retinal rhegmatogenous detachment.Int Ophthalmol. 2021 May;41(5):1709-1716. doi: 10.1007/s10792-021-01729-w. Epub 2021 Jan 28. Int Ophthalmol. 2021. PMID: 33511514
-
Scleral Buckling Alone or in Combination with Pars Plana Vitrectomy for Rhegmatogenous Retinal Detachment Repair: A Meta-Analysis of 7,212 Eyes.Ophthalmologica. 2022;245(4):296-314. doi: 10.1159/000524888. Epub 2022 May 9. Ophthalmologica. 2022. PMID: 35533652
References
-
- Kwon O.W., Song J.H., Roh M.I. Retinal Detachment and Proliferative Vitreoretinopathy. Dev. Ophthalmol. 2016;55:154–162. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
