

Radiosensitization of Allogenic Subcutaneous C6 Glioma Model with Focused Ultrasound-Induced Mild Hyperthermia
- PMID: 38541684
- PMCID: PMC10971558
- DOI: 10.3390/life14030359
Radiosensitization of Allogenic Subcutaneous C6 Glioma Model with Focused Ultrasound-Induced Mild Hyperthermia
Abstract
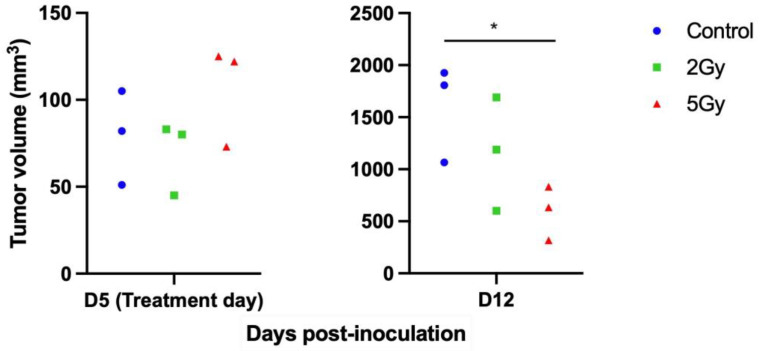
The radiosensitization potential of focused ultrasound (FUS)-induced mild hyperthermia was assessed in an allogenic subcutaneous C6 glioma tumor model in rats. Mild hyperthermia at 42 °C was induced in tumors using a single-element 350 kHz FUS transducer. Radiation was delivered with a small animal radiation research platform using a single-beam irradiation technique. The combined treatment involved 20 min of FUS hyperthermia immediately before radiation. Tumor growth changes were observed one week post-treatment. A radiation dose of 2 Gy alone showed limited tumor control (30% reduction). However, when combined with FUS hyperthermia, there was a significant reduction in tumor growth compared to other treatments (tumor volumes: control-1174 ± 554 mm3, FUS-HT-1483 ± 702 mm3, 2 Gy-609 ± 300 mm3, FUS-HT + 2 Gy-259 ± 186 mm3; ANOVA p < 0.00001). Immunohistological analysis suggested increased DNA damage as a short-term mechanism for tumor control in the combined treatment. In conclusion, FUS-induced mild hyperthermia can enhance the effectiveness of radiation in a glioma tumor model, potentially improving the outcome of standard radiation treatments for better tumor control.
Keywords: focused ultrasound; glioma; hyperthermia; radiosensitization; radiotherapy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



Similar articles
-
Evaluation of a Developed MRI-Guided Focused Ultrasound System in 7 T Small Animal MRI and Proof-of-Concept in a Prostate Cancer Xenograft Model to Improve Radiation Therapy.Cells. 2023 Feb 2;12(3):481. doi: 10.3390/cells12030481. Cells. 2023. PMID: 36766824 Free PMC article.
-
Closed-loop trans-skull ultrasound hyperthermia leads to improved drug delivery from thermosensitive drugs and promotes changes in vascular transport dynamics in brain tumors.Theranostics. 2021 May 24;11(15):7276-7293. doi: 10.7150/thno.54630. eCollection 2021. Theranostics. 2021. PMID: 34158850 Free PMC article.
-
Focused Ultrasound Hyperthermia Augments Release of Glioma-derived Extracellular Vesicles with Differential Immunomodulatory Capacity.Theranostics. 2020 Jun 12;10(16):7436-7447. doi: 10.7150/thno.46534. eCollection 2020. Theranostics. 2020. PMID: 32642004 Free PMC article.
-
Radiosensitization of high-grade gliomas through induced hyperthermia: Review of clinical experience and the potential role of MR-guided focused ultrasound.Radiother Oncol. 2020 Jan;142:43-51. doi: 10.1016/j.radonc.2019.07.017. Epub 2019 Aug 17. Radiother Oncol. 2020. PMID: 31431370 Review.
-
Ultrasound Hyperthermia Technology for Radiosensitization.Ultrasound Med Biol. 2019 May;45(5):1025-1043. doi: 10.1016/j.ultrasmedbio.2018.12.007. Epub 2019 Feb 14. Ultrasound Med Biol. 2019. PMID: 30773377 Free PMC article. Review.
References
-
- Sayan M., Mustafayev T.Z., Sahin B., Kefelioglu E.S.S., Wang S.-J., Kurup V., Balmuk A., Gungor G., Ohri N., Weiner J., et al. Evaluation of Response to Stereotactic Radiosurgery in Patients with Radioresistant Brain Metastases. Radiat. Oncol. J. 2019;37:265–270. doi: 10.3857/roj.2019.00409. - DOI - PMC - PubMed
-
- Niranjan A., Kano H., Iyer A., Kondziolka D., Flickinger J.C., Lunsford L.D. Role of Adjuvant or Salvage Radiosurgery in the Management of Unresected Residual or Progressive Glioblastoma Multiforme in the Pre-Bevacizumab Era. J. Neurosurg. 2015;122:757–765. doi: 10.3171/2014.11.JNS13295. - DOI - PubMed
-
- Xu Z., Marko N.F., Angelov L., Barnett G.H., Chao S.T., Vogelbaum M.A., Suh J.H., Weil R.J. Impact of Preexisting Tumor Necrosis on the Efficacy of Stereotactic Radiosurgery in the Treatment of Brain Metastases in Women with Breast Cancer. Cancer. 2012;118:1323–1333. doi: 10.1002/cncr.26314. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
