

Pulmonary Artery Dilatation Due to Pressure or Volume Overload in Congenital Heart Disease
- PMID: 38541793
- PMCID: PMC10971405
- DOI: 10.3390/jcm13061567
Pulmonary Artery Dilatation Due to Pressure or Volume Overload in Congenital Heart Disease
Abstract
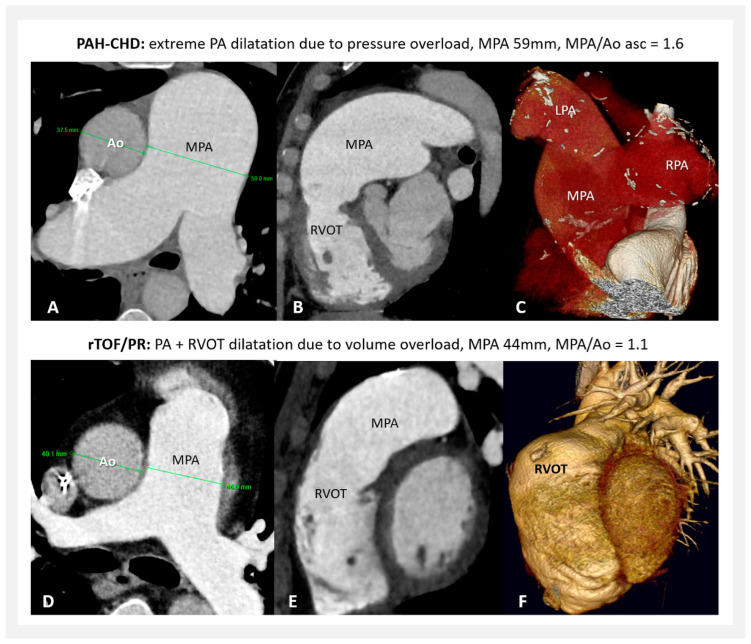
Background: Pulmonary artery dilatation is described mostly in association with pulmonary hypertension. Patients/Methods: Study analysis: 60 patients with pulmonary arterial hypertension in congenital heart disease (PAH-CHD); 64 with repaired tetralogy of Fallot/pulmonary regurgitation (rTOF/PR); and 80 healthy (NORMAL). Measured were: main pulmonary artery (MPA) diameter and MPA/ascending aorta (Ao asc) ratio, by echocardiography (ECHO) and computer tomography or magnetic resonance imaging (CT/MRI). Results: In MPA diameter, significant differences between PAH-CHD, rTOF/PR, and NORMAL were found (median): 37 vs. 27 vs. 21 mm (p < 0.0001). In MPA/Ao asc ratio, there was a difference between PAH-CHD and NORMAL (median): 1.3 vs. 0.8 (p < 0.0001), but not between rTOF/PR and NORMAL: 0.74 vs. 0.8 (p = 0.3). Significant MPA dilatation (>40 mm) was present: in PAH-CHD, 35% (ECHO) and 76.9% (CT/MRI) of patients, while in rTOF/PR, 3.1% (ECHO) and 7.8% (CT/MRI). Severe MPA dilatation (>50 mm) occurred only in PAH-CHD: 16.7% (ECHO) and 31.4% (CT/MRI), while not in rTOF/PR. There was a significant correlation between ECHO and CT/MRI measurements, but ECHO was underestimated in all parameters. Conclusions: MPA dilatation due to pressure overload is more frequent and more severe; volume overload also leads to MPA dilatation but is less severe. The MPA/Ao asc ratio is not reliable for MPA dilatation estimation in rTOF/PR.
Keywords: pulmonary arterial hypertension; pulmonary artery diameter; pulmonary artery dilatation; pulmonary artery to ascending aorta ratio; pulmonary regurgitation; repaired Tetralogy of Fallot.
Conflict of interest statement
M.K. has received fees from Actelion Pharmaceuticals Ltd., AOP Orphan, outside the submitted work. K.B. has received fees from AOP Orphan, Berlin Chemie—Menarini Group, and Egis outside the submitted work. A.K. declares no conflict of interest. E.D. declares no conflict of interest. J.PM. declares no conflict of interest. F.K. declares no conflict of interest. T.H. has received fees from Sanofi and Novartis outside of the submitted work. A.R. has received fees from Actelion Pharmaceuticals Ltd., AOP Orphan, outside the submitted work. T.V. has received fees from Actelion Pharmaceuticals Ltd., AOP Orphan, outside the submitted work. I.S. has received fees from Actelion Pharmaceuticals Ltd., AOP Orphan, and MSD outside the submitted work.
Figures




References
-
- Truong Q.A., Massaro J.M., Rogers I.S., Mahabadi A.A., Kriegel M.F., Fox C.S., O′Donnell C.J., Hoffmann U. Reference values for normal pulmonary artery dimensions by noncontrast cardiac computed tomography: The Framingham Heart Study. Circ. Cardiovasc. Imaging. 2012;5:147–154. doi: 10.1161/CIRCIMAGING.111.968610. - DOI - PMC - PubMed
-
- Humbert M., Kovacs G., Hoeper M.M., Badagliacca R., Berger R.M., Brida M., Carlsen J., Coats A.J., Escribano-Subias P., Ferrari P., et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 2022;43:3618–3731. doi: 10.1093/eurheartj/ehac237. - DOI - PubMed
-
- Weerakkody Y., Hacking C., Worsley C., Luong D., Botz B., Murphy A. Pulmonary Trunk Dilatation. Reference Article. [(accessed on 22 January 2024)]. Available online: https://radiopaedia.org/articles/pulmonary-trunk-dilatation?lang=us.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
