

Diagnostic Challenges in Hemophagocytic Lymphohistiocytosis, a Rare, Potentially Fatal Disease: Two Case Studies
- PMID: 38541872
- PMCID: PMC10970797
- DOI: 10.3390/jcm13061643
Diagnostic Challenges in Hemophagocytic Lymphohistiocytosis, a Rare, Potentially Fatal Disease: Two Case Studies
Abstract
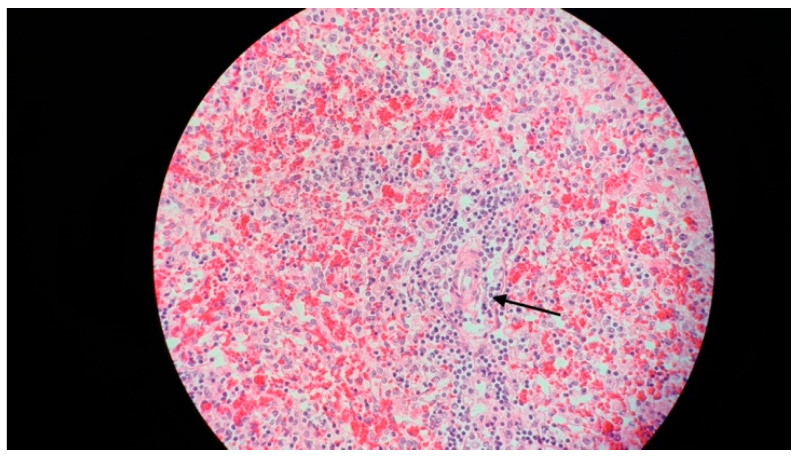
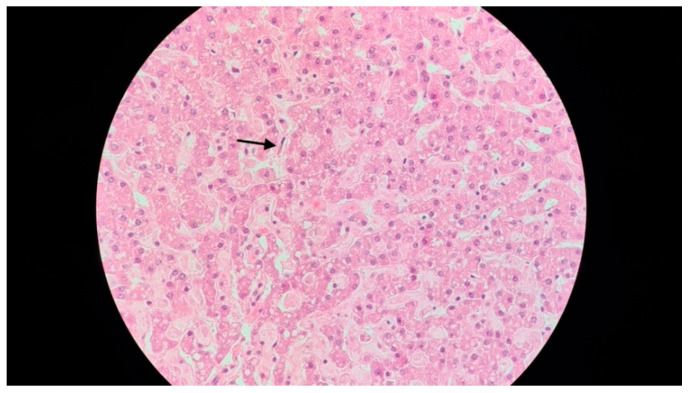
Hemophagocytic lymphohistiocytosis (HLH) is a rare, and potentially fatal, syndrome, characterized by immune system dysregulation, with excessive activation of the macrophages and cytotoxic T cells. It can be classified into primary (genetic) and secondary (acquired) forms. HLH presents with fever, hepatosplenomegaly, cytopenia, and hyperferritinemia, with involvement of various organs. The initial symptoms of HLH are non-specific, but as, if untreated, it can progress rapidly to multiorgan failure, timely diagnosis is essential. We present here two cases of HLH in infants that illustrate the importance of early diagnosis and appropriate treatment, along with a short review of HLH.
Keywords: ferritin; hemophagocytic lymphohistiocytosis; sepsis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




References
-
- Ionescu M.D., Taras R., Dombici B., Balgradean M., Berghea E.C., Nicolescu A. The Challenging Diagnosis of Pediatric Multisystem Inflammatory Syndrome Associated with SARS-CoV-2 Infection-Two Case Reports and Literature Review. J. Pers. Med. 2021;11:318. doi: 10.3390/jpm11040318. - DOI - PMC - PubMed
-
- Jordan M.B., Allen C.E., Greenberg J., Henry M., Hermiston M.L., Kumar A., Hines M., Eckstein O., Ladisch S., Nichols K.E., et al. Challenges in the Diagnosis of Hemophagocytic Lymphohistiocytosis: Recommendations from the North American Consortium for Histiocytosis (NACHO) Pediatr. Blood Cancer. 2019;66:e27929. doi: 10.1002/pbc.27929. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
