

Systemic Vascular Resistance and Myocardial Work Analysis in Hypertrophic Cardiomyopathy and Transthyretin Cardiac Amyloidosis with Preserved Left Ventricular Ejection Fraction
- PMID: 38541896
- PMCID: PMC10970938
- DOI: 10.3390/jcm13061671
Systemic Vascular Resistance and Myocardial Work Analysis in Hypertrophic Cardiomyopathy and Transthyretin Cardiac Amyloidosis with Preserved Left Ventricular Ejection Fraction
Abstract
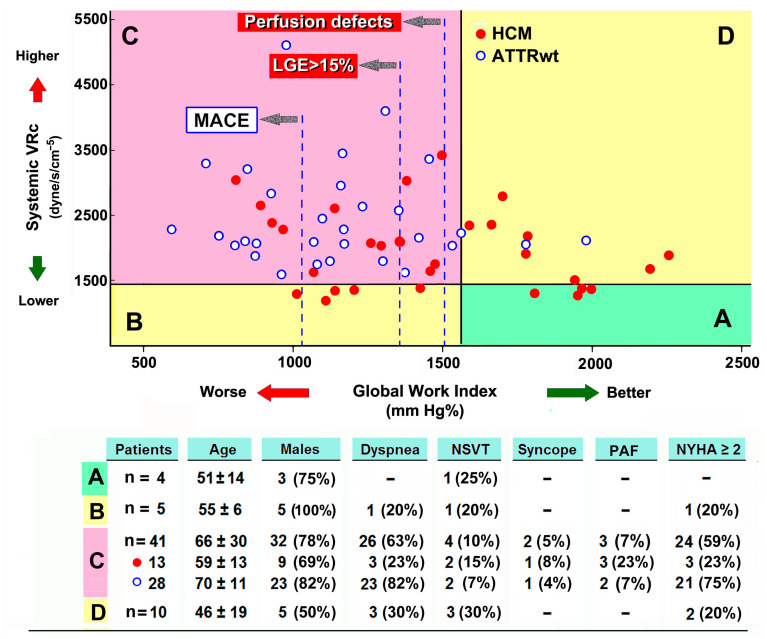
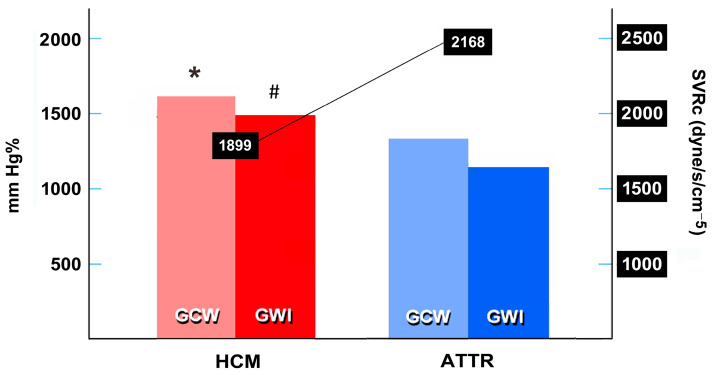
Background: The pathophysiological impact of systemic vascular resistance (SVR) and pressure-strain loop-derived global myocardial work index (GWI) in hypertrophic cardiomyopathy (HCM) and transthyretin cardiac amyloidosis (ATTR) has been randomly investigated. Methods: Both SVR and GWI were assessed in outpatients consecutively referred at two Italian cardiology departments for heart failure with preserved left ventricular ejection fraction (LVEF), affected by either nonobstructive HCM or wild-type ATTR. Based on relevant cross-tabulations, the patients were gathered into 4 functional classes according to cut-off values of 1440 dyne/s/cm-5 for SVR, and 1576 mm Hg% for GWI, as suggested by previous studies. Results: A total of 60 patients, 30 in each group, aged 61 ± 16 years, with 78% males, were studied. HCM patients were younger than those with ATTR and in a better clinical condition (23% HCM vs. 77% ATTR were NYHA class II-III, p < 0.001). Overall, 51 patients (85%) showed a high SVR, 21/30 HCM (70%), and 30 ATTR (100%) (p < 0.005). Both SVR and GWI (expressions of ventricular-arterial coupling) were impaired in 43% of HCM patients (showing greater LV concentric hypertrophy) and 93% of ATTR patients (in advanced NYHA functional class) (p < 0.001). Conclusions: A substantial percentage of present study population showed impaired SVR and/or GWI, despite preserved LVEF. The proposed classification may shed further light on the pathophysiological and clinical characteristics of such hypertrophic phenotypes.
Keywords: cardiac amyloidosis; heart failure with preserved left ventricular ejection fraction; hypertrophic cardiomyopathy; strain echocardiography; systemic vascular resistance; ventricular arterial coupling.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
