

Recent Advances in the Management of Diabetic Kidney Disease: Slowing Progression
- PMID: 38542060
- PMCID: PMC10970506
- DOI: 10.3390/ijms25063086
Recent Advances in the Management of Diabetic Kidney Disease: Slowing Progression
Abstract
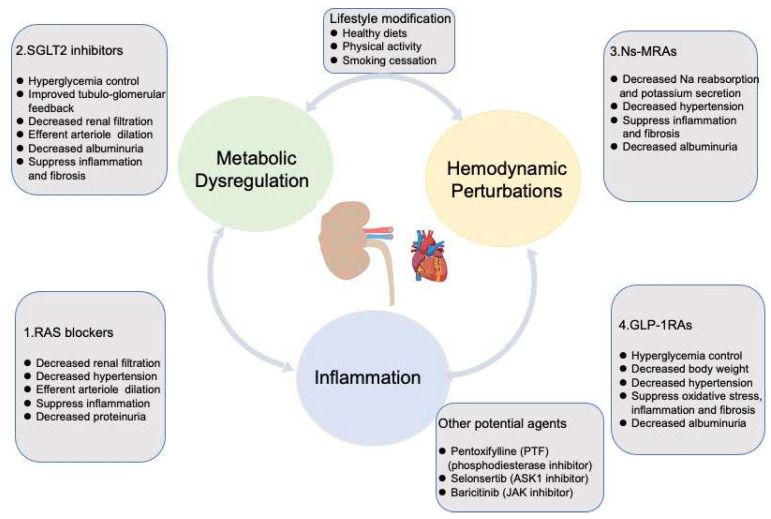
Diabetic kidney disease (DKD) is a major cause of chronic kidney disease (CKD), and it heightens the risk of cardiovascular incidents. The pathogenesis of DKD is thought to involve hemodynamic, inflammatory, and metabolic factors that converge on the fibrotic pathway. Genetic predisposition and unhealthy lifestyle practices both play a significant role in the development and progression of DKD. In spite of the recent emergence of angiotensin receptors blockers (ARBs)/angiotensin converting enzyme inhibitor (ACEI), sodium-glucose cotransporter 2 (SGLT2) inhibitors, and nonsteroidal mineralocorticoid receptors antagonists (NS-MRAs), current therapies still fail to effectively arrest the progression of DKD. Glucagon-like peptide 1 receptor agonists (GLP-1RAs), a promising class of agents, possess the potential to act as renal protectors, effectively slowing the progression of DKD. Other agents, including pentoxifylline (PTF), selonsertib, and baricitinib hold great promise as potential therapies for DKD due to their anti-inflammatory and antifibrotic properties. Multidisciplinary treatment, encompassing lifestyle modifications and drug therapy, can effectively decelerate the progression of DKD. Based on the treatment of heart failure, it is recommended to use multiple drugs in combination rather than a single-use drug for the treatment of DKD. Unearthing the mechanisms underlying DKD is urgent to optimize the management of DKD. Inflammatory and fibrotic factors (including IL-1, MCP-1, MMP-9, CTGF, TNF-a and TGF-β1), along with lncRNAs, not only serve as diagnostic biomarkers, but also hold promise as therapeutic targets. In this review, we delve into the potential mechanisms and the current therapies of DKD. We also explore the additional value of combing these therapies to develop novel treatment strategies. Drawing from the current understanding of DKD pathogenesis, we propose HIF inhibitors, AGE inhibitors, and epigenetic modifications as promising therapeutic targets for the future.
Keywords: biomarkers; chronic kidney disease; diabetic kidney disease; molecular mechanisms; therapies.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
- 82370728/National Natural Science Foundation of China
- 81974096/National Natural Science Foundation of China
- 81974097/National Natural Science Foundation of China
- 82170773/National Natural Science Foundation of China
- 82100729/National Natural Science Foundation of China
- 82200808/National Natural Science Foundation of China
- 82200841/National Natural Science Foundation of China
- 82300843/National Natural Science Foundation of China
- 82300786/National Natural Science Foundation of China
- 2021YFC2500200/National Key Research and Development Program of China
- 2023BCB034/Key Research and Development Program of Hubei Province
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
