

Healthy weight loss maintenance with exercise, GLP-1 receptor agonist, or both combined followed by one year without treatment: a post-treatment analysis of a randomised placebo-controlled trial
- PMID: 38544798
- PMCID: PMC10965408
- DOI: 10.1016/j.eclinm.2024.102475
Healthy weight loss maintenance with exercise, GLP-1 receptor agonist, or both combined followed by one year without treatment: a post-treatment analysis of a randomised placebo-controlled trial
Abstract
Background: New obesity medications result in large weight losses. However, long-term adherence in a real-world setting is challenging, and termination of obesity medication results in weight regain towards pre-treatment body weight. Therefore, we investigated whether weight loss and improved body composition are sustained better at 1 year after termination of active treatment with glucagon-like peptide-1 (GLP-1) receptor agonist, supervised exercise program, or both combined for 1 year.
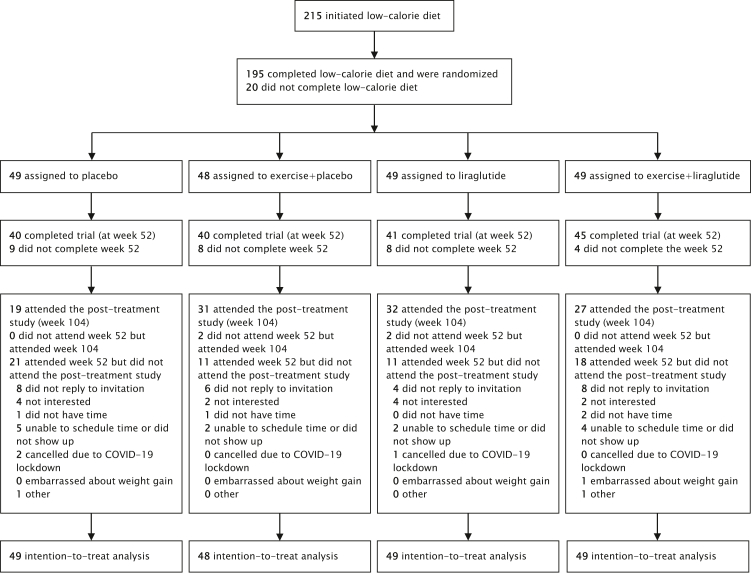
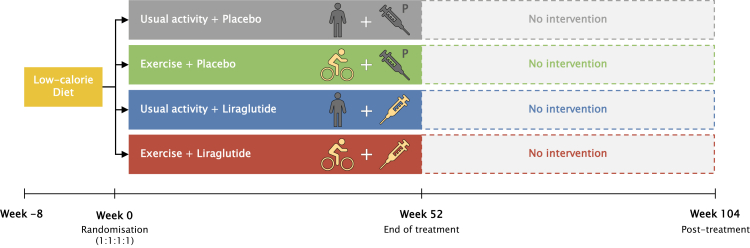
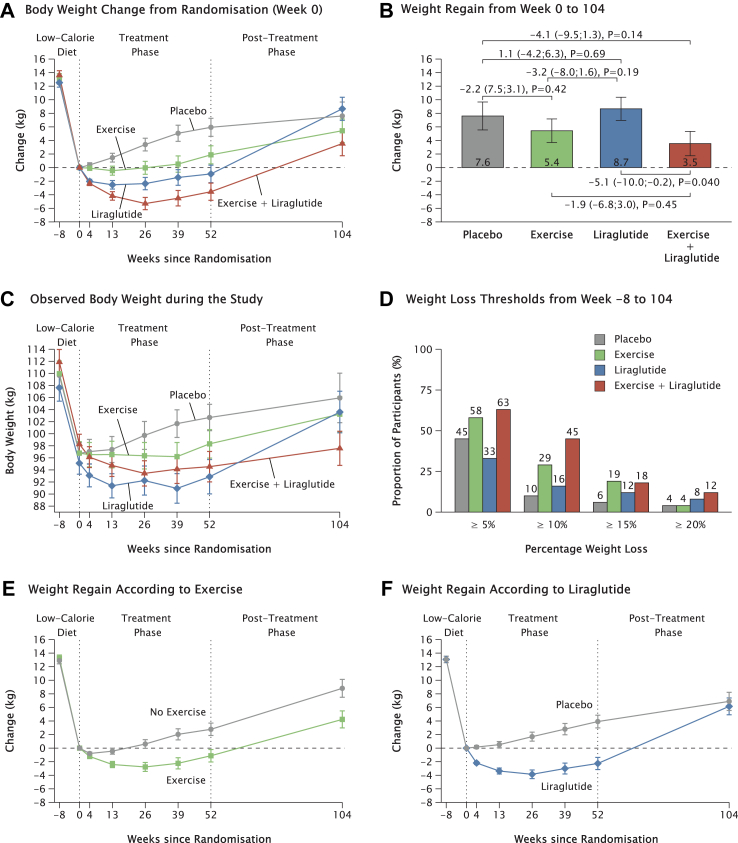
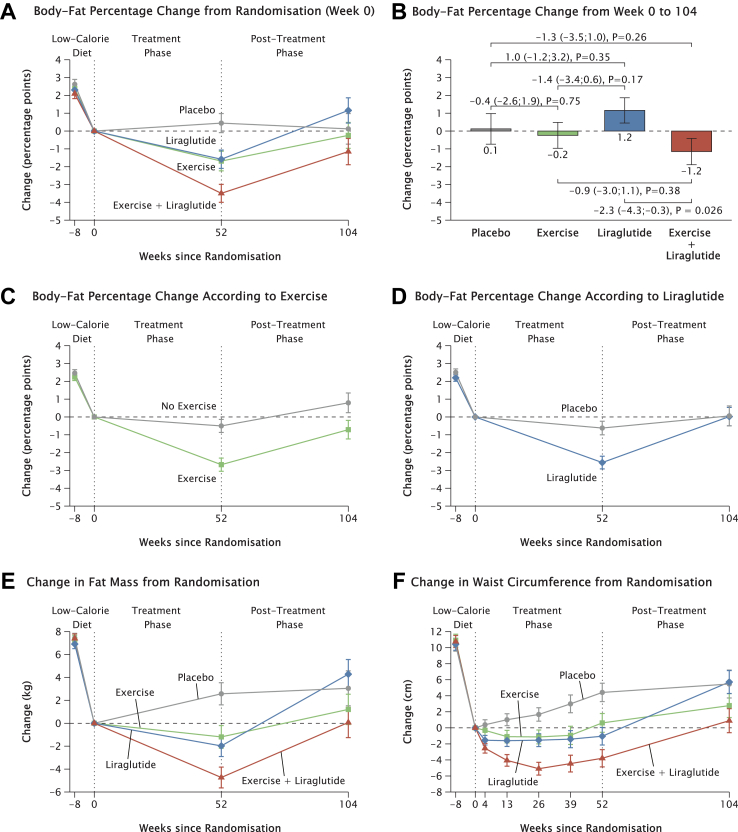
Methods: We conducted a post-treatment study in extension of a randomised, controlled trial in Copenhagen. Adults with obesity (aged 18-65 years and initial body mass index 32-43 kg/m2) completed an eight-week low-calorie diet-induced weight loss of 13.1 kg (week -8 to 0) and were randomly allocated (1:1:1:1) to one-year weight loss maintenance (week 0-52) with either supervised exercise, the GLP-1 receptor agonist once-daily subcutaneous liraglutide 3.0 mg, the combination of exercise and liraglutide, or placebo. 166 Participants completed the weight loss maintenance phase. All randomised participants were invited to participate in the post-treatment study with outcome assessments one year after treatment termination, at week 104. The primary outcome of the post-treatment assessment was change in body weight from after the initial weight loss (at randomisation, week 0) to one year after treatment termination (week 104) in the intention-to-treat population. The secondary outcome was change in body-fat percentage (week 0-104). The study is registered with EudraCT, 2015-005585-32, and with ClinicalTrials.gov, NCT04122716.
Findings: Between Dec 17, 2018, and Dec 17, 2020, 109 participants attended the post-treatment study. From randomisation to one year after termination of combined exercise and liraglutide treatment (week 0-104), participants had reduced body weight (-5.1 kg [95% CI -10.0; -0.2]; P = 0.040) and body-fat percentage (-2.3%-points [-4.3 to -0.3]; P = 0.026) compared with after termination of liraglutide alone. More participants who had previously received combination treatment maintained a weight loss of at least 10% of initial body weight one year after treatment termination (week -8 to 104) compared with participants who had previously received placebo (odds ratio [OR] 7.2 [2.4; 21.3]) and liraglutide (OR 4.2 [1.6; 10.8]). More participants who had previously received supervised exercise maintained a weight loss of at least 10% compared with placebo (OR 3.7 [1.2; 11.1]). During the year after termination of treatment (week 52-104), weight regain was 6.0 kg [2.1; 10.0] larger after termination of liraglutide compared with after termination of supervised exercise and 2.5 kg [-1.5 to 6.5] compared with after termination of combination treatment.
Interpretation: The addition of supervised exercise to obesity pharmacotherapy seems to improve healthy weight maintenance after treatment termination compared with treatment termination of obesity pharmacotherapy alone. Body weight and body composition were maintained one year after termination of supervised exercise, in contrast to weight regain after termination of treatment with obesity pharmacotherapy alone.
Funding: Helsefonden and the Novo Nordisk Foundation.
Keywords: Exercise; GLP-1 receptor agonist; Obesity; Physical activity; Weight loss maintenance.
© 2024 The Authors.
Conflict of interest statement
RMS: family member owns Novo Nordisk stocks. S.M.: Advisory boards: AstraZeneca; Boehringer Ingelheim; Eli Lilly; Merck Sharp & Dohme; Novo Nordisk; Sanofi Aventis. Lecture fees: AstraZeneca; Boehringer Ingelheim; Merck Sharp & Dohme; Novo Nordisk; Sanofi Aventis. Research Grant Recipient: Novo Nordisk, Boehringer-Ingelheim. S.S.T.: Research Grant and Lecture Fee Recipient: Novo Nordisk. J.J.H.: Advisory board: Novo Nordisk. M.B.B.: Research Grant Novo Nordisk A/S, payment made to institution. B.M.S.: Board member of Steno Diabetes Center Copenhagen. Board member of the Centre for Childhood Health, appointed by the Novo Nordisk Foundation.
Figures
References
-
- Avila C., Holloway A.C., Hahn M.K., et al. An overview of links between obesity and mental health. Curr Obes Rep. 2015;4(3):303–310. - PubMed
-
- Narayan K.M.V., Boyle J.P., Thompson T.J., Gregg E.W., Williamson D.F. Effect of BMI on lifetime risk for diabetes in the U.S. Diabetes Care. 2007;30(6):1562–1566. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
