

Neurophysiological trajectories in Alzheimer's disease progression
- PMID: 38546337
- PMCID: PMC10977971
- DOI: 10.7554/eLife.91044
Neurophysiological trajectories in Alzheimer's disease progression
Abstract
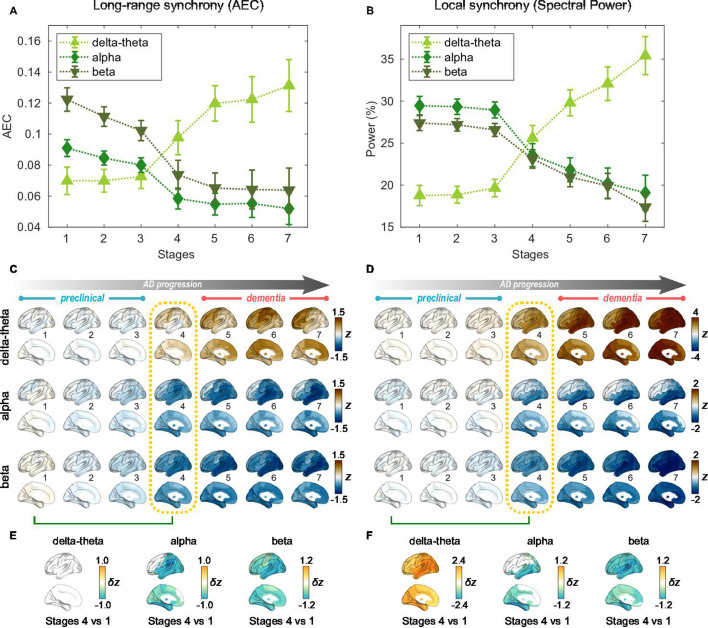
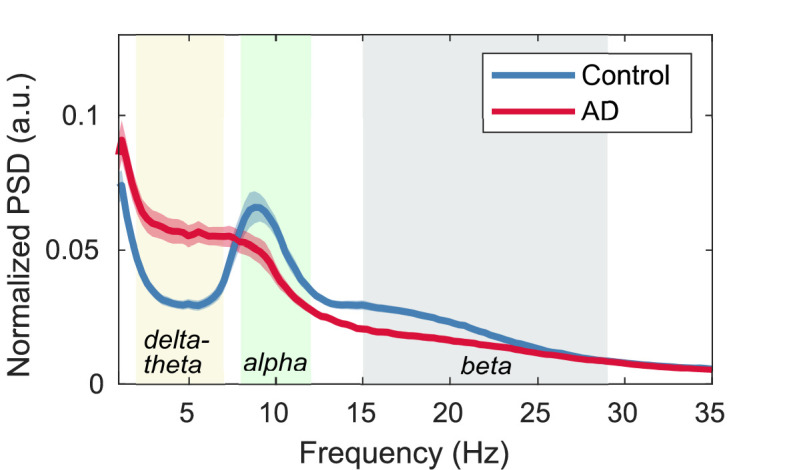
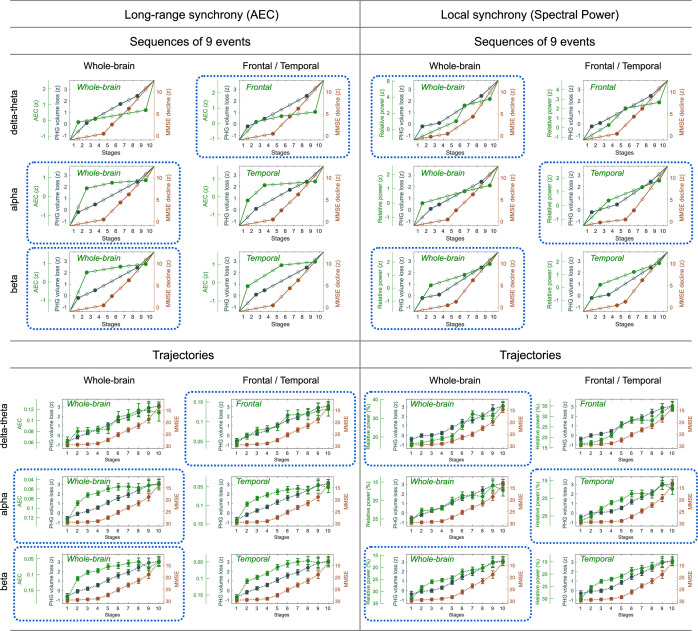
Alzheimer's disease (AD) is characterized by the accumulation of amyloid-β and misfolded tau proteins causing synaptic dysfunction, and progressive neurodegeneration and cognitive decline. Altered neural oscillations have been consistently demonstrated in AD. However, the trajectories of abnormal neural oscillations in AD progression and their relationship to neurodegeneration and cognitive decline are unknown. Here, we deployed robust event-based sequencing models (EBMs) to investigate the trajectories of long-range and local neural synchrony across AD stages, estimated from resting-state magnetoencephalography. The increases in neural synchrony in the delta-theta band and the decreases in the alpha and beta bands showed progressive changes throughout the stages of the EBM. Decreases in alpha and beta band synchrony preceded both neurodegeneration and cognitive decline, indicating that frequency-specific neuronal synchrony abnormalities are early manifestations of AD pathophysiology. The long-range synchrony effects were greater than the local synchrony, indicating a greater sensitivity of connectivity metrics involving multiple regions of the brain. These results demonstrate the evolution of functional neuronal deficits along the sequence of AD progression.
Keywords: Alzheimer's disease; biomarkers; electrophysiology; functional connectivity; human; magnetoencephalography; neuroscience.
© 2023, Kudo, Ranasinghe et al.
Conflict of interest statement
KK KK is a full-time employee of Ricoh Company, Ltd, KR, FS, KR, BM, JK, GR, KV, HK No competing interests declared, HM HM is a full-time employee of Ricoh Company, Ltd, KS KS is an employee of Signal Analysis Inc, SN SSN is a scientific consultant to MEGIN Inc. and a Medical Strategy Adviser to Hippoclinic Inc. He served on the scientific advisory board for Rune Labs Inc. from 2019-2022. He was the recipient of an industry contract from Ricoh MEG USA Inc
Figures











Update of
-
Neurophysiological trajectories in Alzheimer's disease progression.bioRxiv [Preprint]. 2024 Mar 8:2023.05.18.541379. doi: 10.1101/2023.05.18.541379. bioRxiv. 2024. Update in: Elife. 2024 Mar 28;12:RP91044. doi: 10.7554/eLife.91044. PMID: 37293044 Free PMC article. Updated. Preprint.
References
-
- Ablin P, Cardoso JF, Gramfort A. Faster independent component analysis by preconditioning with hessian approximations. IEEE Transactions on Signal Processing. 2018;66:4040–4049. doi: 10.1109/TSP.2018.2844203. - DOI
-
- Ahnaou A, Moechars D, Raeymaekers L, Biermans R, Manyakov NV, Bottelbergs A, Wintmolders C, Van Kolen K, Van De Casteele T, Kemp JA, Drinkenburg WH. Emergence of early alterations in network oscillations and functional connectivity in a tau seeding mouse model of Alzheimer’s disease pathology. Scientific Reports. 2017;7:14189. doi: 10.1038/s41598-017-13839-6. - DOI - PMC - PubMed
-
- Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, Gamst A, Holtzman DM, Jagust WJ, Petersen RC, Snyder PJ, Carrillo MC, Thies B, Phelps CH. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging‐Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s & Dementia. 2011;7:270–279. doi: 10.1016/j.jalz.2011.03.008. - DOI - PMC - PubMed
-
- Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. Journal of the Royal Statistical Society. 1995;57:289–300. doi: 10.1111/j.2517-6161.1995.tb02031.x. - DOI
MeSH terms
Substances
Grants and funding
- P30AG062422/NH/NIH HHS/United States
- K23 AG038357/AG/NIA NIH HHS/United States
- R21 AG077498/AG/NIA NIH HHS/United States
- P30 AG062422/AG/NIA NIH HHS/United States
- K08AG058749/NH/NIH HHS/United States
- RF1 AG062196/AG/NIA NIH HHS/United States
- P50DC019900/NH/NIH HHS/United States
- R01AG062196/NH/NIH HHS/United States
- K23AG038357/NH/NIH HHS/United States
- R01 DC017091/DC/NIDCD NIH HHS/United States
- R21AG077498/NH/NIH HHS/United States
- R01DC017091/NH/NIH HHS/United States
- K08 AG058749/AG/NIA NIH HHS/United States
- R01NS100440/NH/NIH HHS/United States
- P50 DC019900/DC/NIDCD NIH HHS/United States
- R01 NS100440/NS/NINDS NIH HHS/United States
- PCTRB-13-288476 made possible by Part the CloudTM/ALZ/Alzheimer's Association/United States
- AARG-21-849773/ALZ/Alzheimer's Association/United States
