

Acellular Dermal Matrix-Assisted Tissue Expansion for Giant Congenital Melanocytic Nevi of the Extremities and Trunk in Pediatric Patients
- PMID: 38546404
- PMCID: PMC11651352
- DOI: 10.1097/PRS.0000000000011434
Acellular Dermal Matrix-Assisted Tissue Expansion for Giant Congenital Melanocytic Nevi of the Extremities and Trunk in Pediatric Patients
Abstract
Background: Tissue expansion for treating giant congenital melanocytic nevi (GCMN) is a commonly used surgical method. However, the procedure's efficacy is often hindered by anatomical and histologic characteristics and blood supply, particularly in the extremities and trunk. Enhancing expansion efficiency while reducing complications is thus a topic to be investigated, especially for pediatric patients undergoing rapid physical and psychological development with higher risks of noncompliance to medical instructions. The purpose of this study was to explore the effectiveness of expansion in extremities and trunk by immobilizing the acellular dermal matrix (ADM) in the gravitational force zone of inflating expanders.
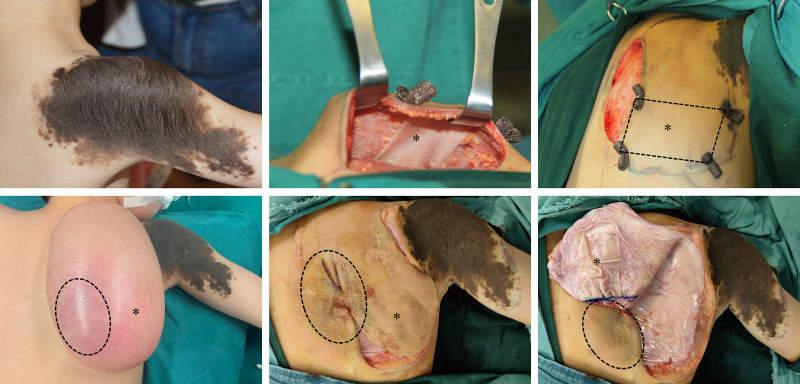
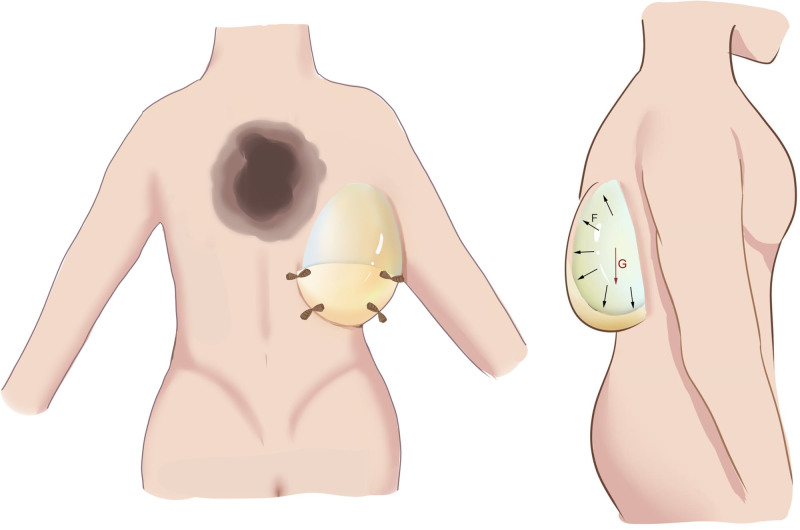
Methods: All patients involved in this research underwent ADM-assisted tissue expansion in either the extremities or trunk. ADM was fully flattened, securely fixed to the lower pole of the expander, and subsequently attached to the inner surface of the expanding flap.
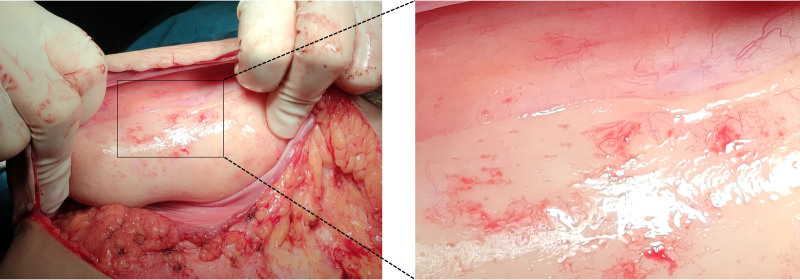
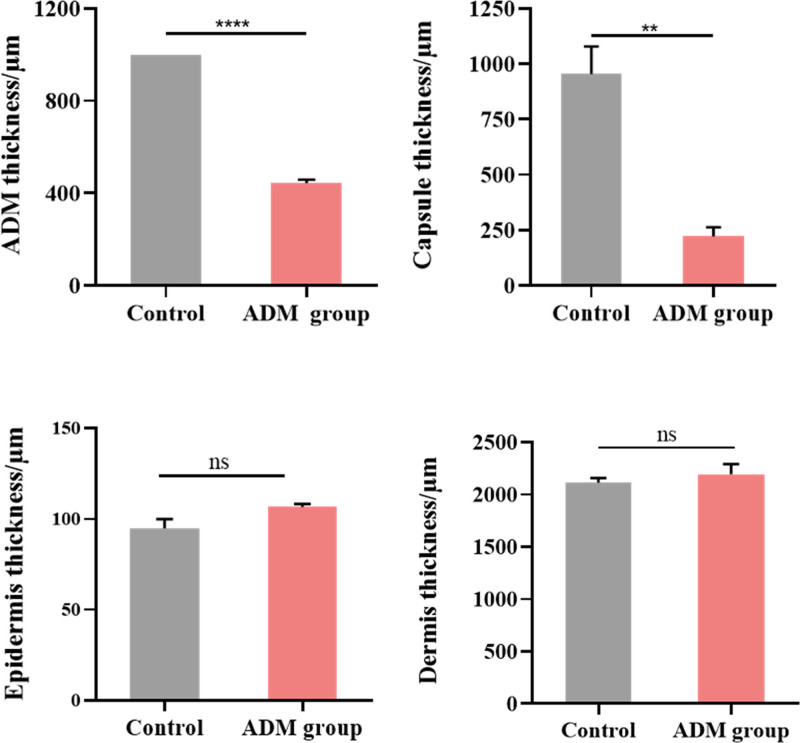
Results: From 2021 to 2023, a total of 9 pediatric patients with GCMN underwent ADM-assisted tissue expansion. All patients achieved the desired expansion volume without experiencing petechiae, ecchymosis, or skin ulceration in the ADM-covered area. The process was well tolerated by all patients, with no reports of itching, pain, allergic reaction, or fever. During the flap transfer, the ADM was observed to be firmly adhered to the expanding flap with discernible capillary network.
Conclusions: ADM-assisted tissue expansion demonstrates promise in augmenting expansion efficiency and reducing the time needed for surgical intervention in the extremities and trunk, thereby presenting significant clinical value for pediatric patients with GCMN.
Clinical question/level of evidence: Therapeutic, IV.
Copyright © 2024 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the American Society of Plastic Surgeons.
Conflict of interest statement
The authors have no financial interest to declare in relation to the content of this article.
Figures


Similar articles
-
Autologous skin reconstruction by combining epidermis and acellular dermal matrix tissue derived from the skin of giant congenital melanocytic nevi.J Artif Organs. 2013 Sep;16(3):332-42. doi: 10.1007/s10047-013-0708-2. Epub 2013 May 5. J Artif Organs. 2013. PMID: 23644894
-
The feasibility of tissue expanders in reconstruction of giant congenital melanocytic nevi in children.Surg Innov. 2010 Sep;17(3):189-94. doi: 10.1177/1553350610371627. Epub 2010 May 31. Surg Innov. 2010. PMID: 20513722
-
Refinements in the Preexpanded Distant Flap for Giant Melanocytic Nevi of the Upper Extremity in Pediatric Patients.Plast Reconstr Surg. 2024 Aug 1;154(2):375-383. doi: 10.1097/PRS.0000000000010734. Epub 2023 May 23. Plast Reconstr Surg. 2024. PMID: 37220387
-
Treatment of a giant congenital melanocytic nevus in the adult: review of the current management of giant congenital melanocytic nevus.Ann Plast Surg. 2015 May;74 Suppl 1:S57-61. doi: 10.1097/SAP.0000000000000433. Ann Plast Surg. 2015. PMID: 25664413 Review.
-
Treatment of large and giant nevi.Clin Plast Surg. 2005 Jan;32(1):11-8, vii. doi: 10.1016/j.cps.2004.08.004. Clin Plast Surg. 2005. PMID: 15636760 Review.
References
-
- Radovan C. Breast reconstruction after mastectomy using the temporary expander. Plast Reconstr Surg. 1982;69:195–208. - PubMed
-
- Azzi JL, Thabet C, Azzi AJ, Gilardino MS. Complications of tissue expansion in the head and neck. Head Neck 2020;42:747–762. - PubMed
-
- Donelan MB, Bojovic B. Reconstruction of the head and neck after burns. In: Herndon DN, ed. Total Burn Care. 5th ed. Edinburgh: Elsevier; 2018:532–554.e531.
-
- Khalatbari B, Bakhshaeekia A. Ten-year experience in face and neck unit reconstruction using tissue expanders. Burns 2013;39:522–527. - PubMed
-
- Ding Y, Huang X, Wang Y, et al. . Reconstruction of facial multiunit defects using expanded scalp flap with laser depilation in a group of predominantly pediatric patients. Facial Plast Surg Aesthet Med. 2022;24:352–356. - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
