

Case Reports
doi: 10.3324/haematol.2023.284917.
BCMA x CD3 T-cell engager in a patient with pentarefractory multiple myeloma and HIV: a clinical and immunological report
Affiliations
- PMID: 38546668
- PMCID: PMC11367224
- DOI: 10.3324/haematol.2023.284917
Item in Clipboard
Case Reports
BCMA x CD3 T-cell engager in a patient with pentarefractory multiple myeloma and HIV: a clinical and immunological report
Haematologica.
.
No abstract available
Figures

Clinical course before and after teclistamab initiation. (A) Clinical events and laboratory parameters before and after initiation of teclistamab therapy. (B) High-sensitive HIV-1 RNA polymerase chain reaction and cytomegalovirus (CMV) DNA polymerase chain reaction results. Open symbols indicate values below the lower limit of detection. DVd: daratumumab, bortezomib, dexamethasone; PCd: pomalidomide, cyclophosphamide, dexamethasone; Isa-KCd: isatuximab, carfilzomib, cyclophosphamide, dexamethasone; VTd-PACE: bortezomib, thalidomide, dexamethasone, cisplatin, doxorubicin, cyclophosphamide, etoposide; Ig: immunglobulin.

Characterization of peripheral blood T cells before and during teclistamab therapy. (A) Elevated CD8:CD4 ratio, (B) high frequencies of late differentiated CD8+ T cells and (C) regulatory CD4+ T cells are present in the pretreatment samples of the described patient (red arrows) as positive and negative prognostic markers for teclistamab response, and correspond to immunological changes typically observed in people with human immunodeficiency virus (HIV). (D) The CD8+ T-cell memory phenotype is skewed towards an effector memory and a terminally differentiated phenotype and marked by loss of naïve T cells. (E) Peripheral blood CD8+ T cells were highly activated 1 and 2 months after treatment initiation, as indicated by CD38 and HLA-DR co-expression. The result from 5 months before treatment initiation (*) is most likely underestimated due to anti-CD38 pretreatment. (F) Circulating CD8+ T cells showed high cytolytic (granzyme B+ perforin+) response frequencies. (G) The expression of the immune checkpoint molecules PD-1, TIGIT, and TIM-3 is slightly elevated on CD8+ T cells of patients with HIV (PWH) compared to HIV-negative controls (HIV-). (H) Expression of PD-1, TIGIT, and TIM-3 on CD8+ T cells peaked 1 month after teclistamab initiation in the described patient. For the respective analyses, the results of each N=7 HIV-positive (HIV+) and HIV- controls are displayed as median with interquartile range or mean (bar charts). TEM: effector memory T cells; TEMRA: terminally differentiated T cells; TREG: regulatory T cells; TCM: central memory T cells; TN: naïve T cells.
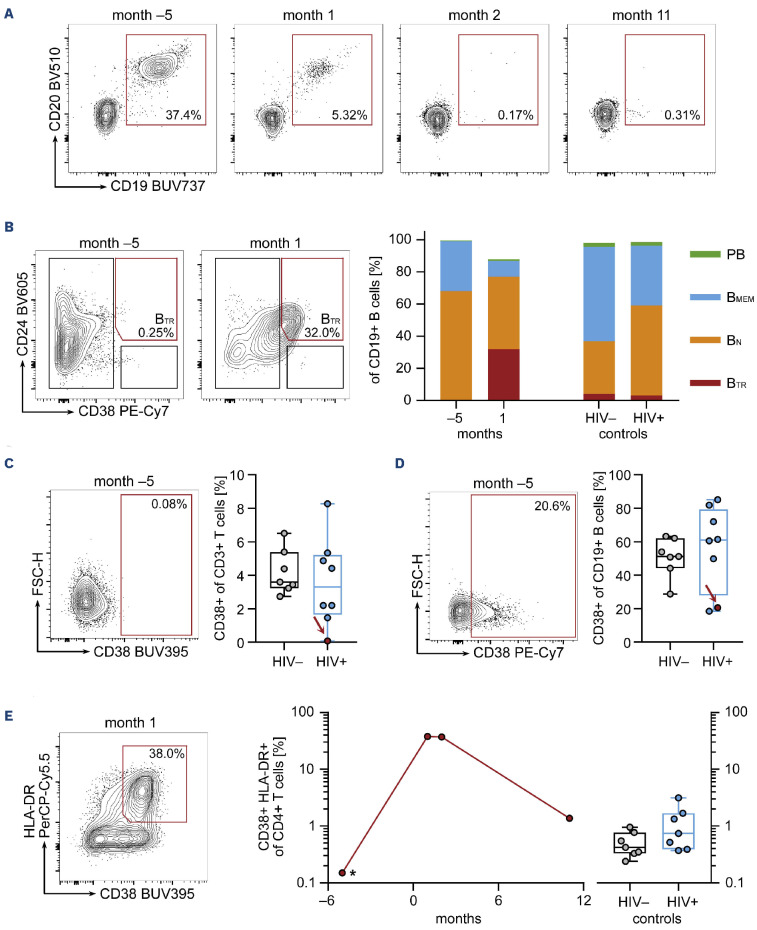
Teclistamab-associated changes in the B-cell compartment and CD4+ T-cell activation. (A) CD19+ B cells disappeared from peripheral blood samples during teclistamab therapy. Gated on viable, CD14-, CD3- single lymphocytes. (B) One month after therapy initiation, the phenotype of the remaining B cells shifted towards a predominant CD24+ CD38high transitional phenotype. (C) Depletion of CD38+ T cells and (D) CD38+ B cells due to anti-CD38 treatment before teclistamab therapy. (E) Peripheral blood CD4+ T cells were highly activated 1 and 2 months after treatment initiation, as indicated by CD38 and HLA-DR co-expression. The result from 5 months before treatment initiation (*) is most likely underestimated due to anti-CD38 pretreatment. The results of each N=7 human immunodeficiency virus (HIV)-positive (HIV+) and HIV-negative (HIV-) controls are displayed as median with interquartile range or mean (bar charts).BMEM: memory B cells; BN: naïve B cells; BTR: transitional B cells; PB: plasmablasts.
References
-
- Moreau P, Kumar SK, San Miguel J, et al. . Treatment of relapsed and refractory multiple myeloma: recommendations from the International Myeloma Working Group. Lancet Oncol. 2021;22(3):e105-e118. - PubMed
-
- Moreau P, van de Donk NWCJ, Delforge M, et al. . Comparative efficacy of teclistamab versus current treatments in real-world clinical practice in the Prospective LocoMMotion Study in patients with triple-class-exposed relapsed and/or refractory multiple myeloma. Adv Ther. 2023;40(5):2412-2425. - PMC - PubMed
-
- Hattenhauer ST, Mispelbaum R, Hentrich M, Boesecke C, Monin MB. Enabling CAR T-cell therapies for HIV-positive lymphoma patients - A call for action. HIV Med. 2023;24(9):957-964. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
