

Comparable rates of lumbar disc degeneration at long-term following adolescent idiopathic scoliosis spinal fusion extended to L3 or L4: systematic review and meta-analysis
- PMID: 38546965
- PMCID: PMC11217089
- DOI: 10.1007/s43390-024-00849-4
Comparable rates of lumbar disc degeneration at long-term following adolescent idiopathic scoliosis spinal fusion extended to L3 or L4: systematic review and meta-analysis
Abstract
Purpose: Surgical treatment of adolescent idiopathic scoliosis (AIS) requires a careful choice of fusion levels. The usual recommendation for the selection of the lowest instrumented vertebra (LIV) for double major or thoracolumbar/lumbar (TL/L) curves falls on L3 or L4. The aim of the present study is to assess if the spinal fusion with LIV selection of L3 or L4 in AIS patients has a clinical or radiological impact in terms of degenerative disc disease (DDD) in distal unfused segments at long-term follow-up.
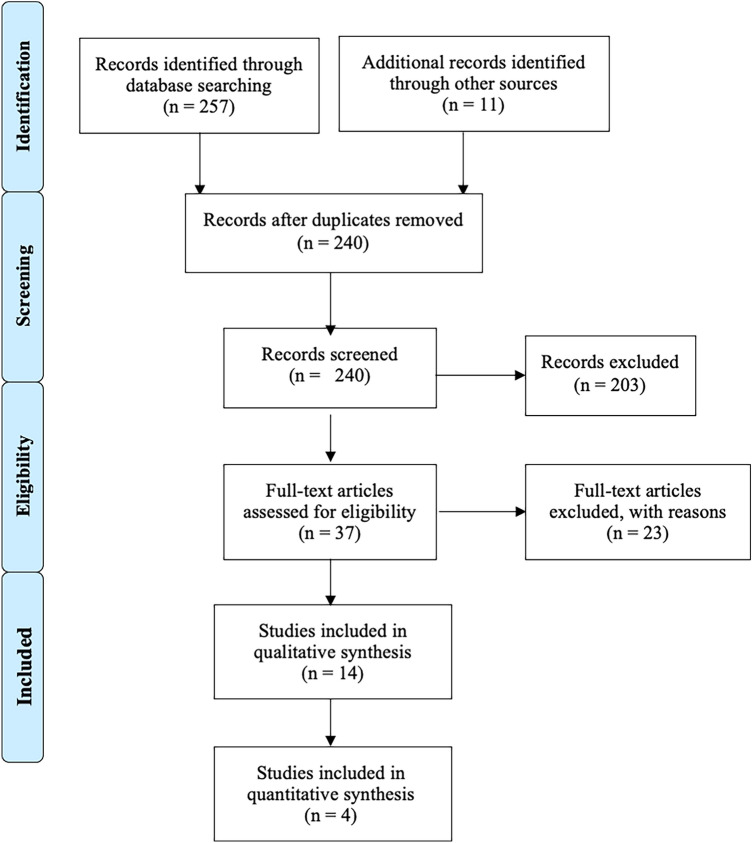
Methods: A systematic search of electronic databases from eligible articles was conducted. Only studies regarding long-term follow-up of AIS patients treated with spinal fusion were included. Clinical and radiographic outcomes were extracted and summarized. Meta-analysis on long-term follow-up MRI studies was performed. p value < 0.05 was considered significant.
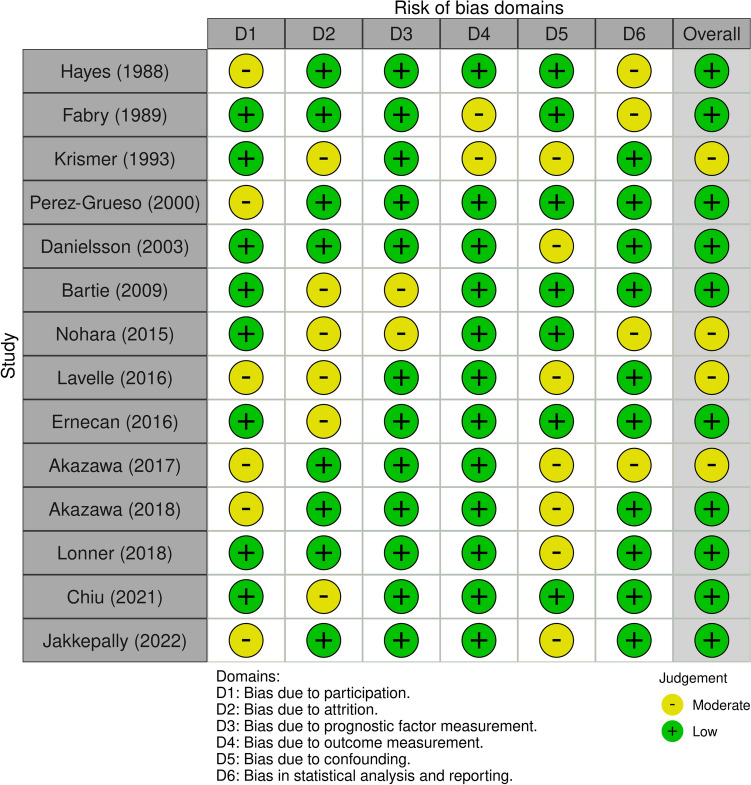
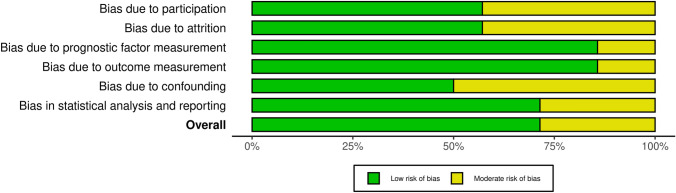
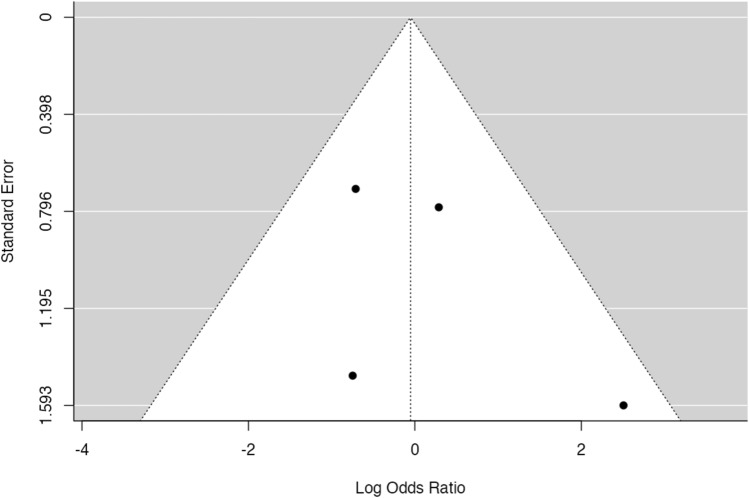
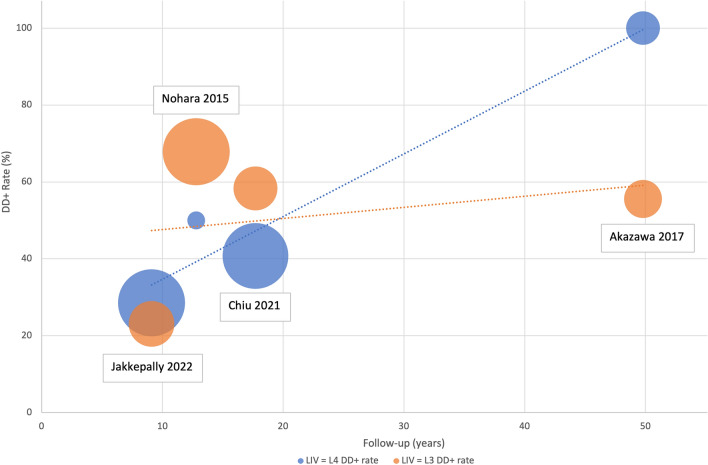
Results: Fourteen studies were included, for a total of 1264 patients. Clinical assessment of included patients showed a slight tendency to have worse clinical outcomes if spinal fusion is extended to L4 rather than L3. Despite that, meta-analysis could not be performed on clinical parameters because of heterogeneity of evaluated PROMs in included studies. Magnetic resonance imaging (MRI) evaluation at long-term follow-up showed no significant difference in terms of disc degeneration rate at overall meta-analysis (p = 0.916) between patients fused to L3 and L4.
Conclusion: The LIV selection of L3 rather than L4, according to current literature, does not prevent disc degeneration in distal unfused segments over the long term. Long-term studies of patients treated with contemporary spinal instrumentation are needed.
Keywords: Adjacent segment disease; Adolescent idiopathic scoliosis; Degenerative disc disease; LIV; Pedicle screw; Spinal fusion.
© 2024. The Author(s).
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose.
Figures

Similar articles
-
Resolution of the lumbosacral fractional curve and evaluation of the risk for adding on in 101 patients with posterior correction of Lenke 3, 4, and 6 curves.J Neurosurg Spine. 2021 Jul 30;35(4):471-485. doi: 10.3171/2020.11.SPINE201313. Print 2021 Oct 1. J Neurosurg Spine. 2021. PMID: 35658389
-
Incidence and risk factors of distal adjacent disc degeneration in adolescent idiopathic scoliosis patients undergoing fusion surgery: a systematic review and meta-analysis.Eur Spine J. 2024 Apr;33(4):1624-1636. doi: 10.1007/s00586-024-08165-1. Epub 2024 Feb 19. Eur Spine J. 2024. PMID: 38372794
-
Total disc replacement surgery for symptomatic degenerative lumbar disc disease: a systematic review of the literature.Eur Spine J. 2010 Aug;19(8):1262-80. doi: 10.1007/s00586-010-1445-3. Epub 2010 May 28. Eur Spine J. 2010. PMID: 20508954 Free PMC article.
-
Arthroplasty versus fusion in single-level cervical degenerative disc disease.Cochrane Database Syst Rev. 2012 Sep 12;(9):CD009173. doi: 10.1002/14651858.CD009173.pub2. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2015 May 21;(5):CD009173. doi: 10.1002/14651858.CD009173.pub3. PMID: 22972137 Updated.
-
Patient and surgical predictors of 3D correction in posterior spinal fusion: a systematic review.Eur Spine J. 2023 Jun;32(6):1927-1946. doi: 10.1007/s00586-023-07708-2. Epub 2023 Apr 20. Eur Spine J. 2023. PMID: 37079078
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials