

Long-Term Risk of Reintervention After Surgical Leiomyoma Treatment in an Integrated Health Care System
- PMID: 38547478
- PMCID: PMC11022990
- DOI: 10.1097/AOG.0000000000005557
Long-Term Risk of Reintervention After Surgical Leiomyoma Treatment in an Integrated Health Care System
Abstract
Objective: To compare long-term risk of reintervention across four uterus-preserving surgical treatments for leiomyomas and to assess effect modification by sociodemographic factors in a prospective cohort study in an integrated health care delivery system.
Methods: We studied a cohort of 10,324 patients aged 18-50 (19.9% Asian, 21.2% Black, 21.3% Hispanic, 32.5% White, 5.2% additional races and ethnicities) who had a first uterus-preserving procedure (abdominal, laparoscopic, or vaginal myomectomy [referred to as myomectomy]; hysteroscopic myomectomy; endometrial ablation; uterine artery embolization) after leiomyoma diagnosis in the 2009-2021 electronic health records of Kaiser Permanente Northern California. We followed up patients until reintervention (second uterus-preserving procedure or hysterectomy) or censoring. We used a Kaplan-Meier estimator to calculate the cumulative incidence of reintervention and Cox regression models to estimate hazard ratios and 95% CIs comparing rates of reintervention across procedures, adjusting for age, parity, race and ethnicity, body mass index (BMI), Neighborhood Deprivation Index, and year. We also assessed effect modification by demographic characteristics.
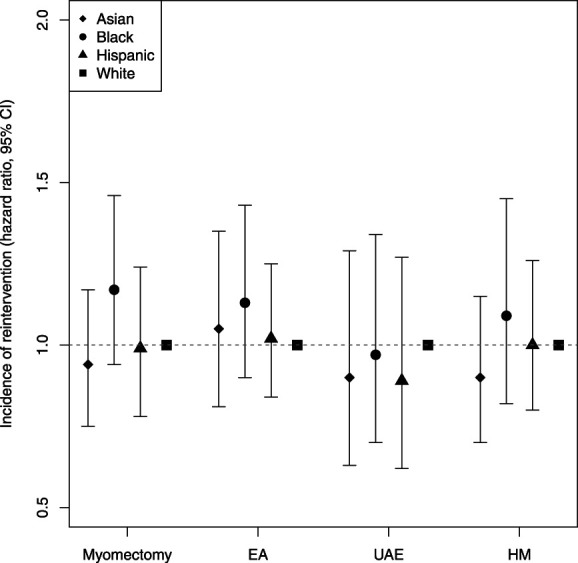
Results: Median follow-up was 3.8 years (interquartile range 1.8-7.4 years). Index procedures were 18.0% (1,857) hysteroscopic myomectomies, 16.2% (1,669) uterine artery embolizations, 21.4% (2,211) endometrial ablations, and 44.4% (4,587) myomectomies. Accounting for censoring, the 7-year reintervention risk was 20.6% for myomectomy, 26.0% for uterine artery embolization, 35.5% for endometrial ablation, and 37.0% for hysteroscopic myomectomy; 63.2% of reinterventions were hysterectomies. Within each procedure type, reintervention rates did not vary by BMI, race and ethnicity, or Neighborhood Deprivation Index. However, rates of reintervention after uterine artery embolization, endometrial ablation, and hysteroscopic myomectomy decreased with age, and reintervention rates for hysteroscopic myomectomy were higher for parous than nulliparous patients.
Conclusion: Long-term reintervention risks for uterine artery embolization, endometrial ablation, and hysteroscopic myomectomy are greater than for myomectomy, with potential variation by patient age and parity but not BMI, race and ethnicity, or Neighborhood Deprivation Index.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Financial Disclosure Lauren Wise is a paid consultant for AbbVie, Inc. She received in-kind donations from Swiss Precision Diagnostics and Kindara.com for primary data collection in PRESTO. She also received payment from The Gates Foundation. The other authors did not report any potential conflicts of interest.
Figures

References
-
- Hartmann KE, Fonnesbeck C, Surawicz T, Krishnaswami S, Andrews JC, Wilson JO, et al. Management of uterine fibroids. Agency for Healthcare Research and Quality; 2017. - PubMed
-
- Sandberg E, Tummers FHMP, Cohen SL, van den Haak L, Dekkers OM, Jansen FW. Reintervention risk and quality of life outcomes after uterine-sparing interventions for fibroids: a systematic review and meta-analysis. Fertil Steril 2018;109:698–707.e1. doi: 10.1016/j.fertnstert.2017.11.033 - DOI - PubMed
