

Increased Intracranial Arterial Pulsatility and Microvascular Brain Damage in Pseudoxanthoma Elasticum
- PMID: 38548304
- PMCID: PMC11288551
- DOI: 10.3174/ajnr.A8212
Increased Intracranial Arterial Pulsatility and Microvascular Brain Damage in Pseudoxanthoma Elasticum
Abstract
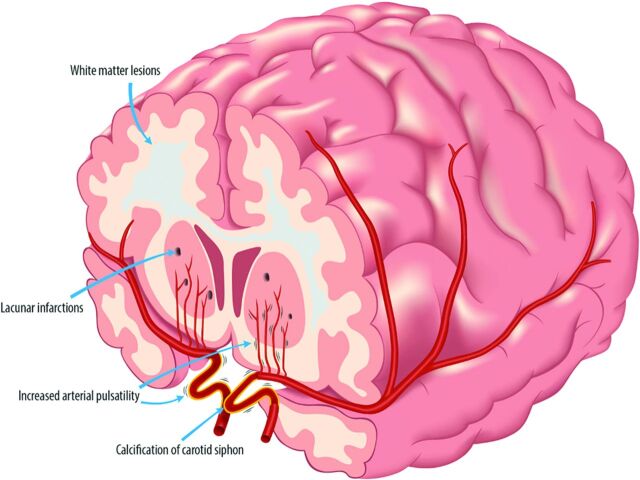
Background and purpose: Carotid siphon calcification might contribute to the high prevalence of cerebrovascular disease in pseudoxanthoma elasticum through increased arterial flow pulsatility. This study aimed to compare intracranial artery flow pulsatility, brain volumes, and small-vessel disease markers between patients with pseudoxanthoma elasticum and controls and the association between arterial calcification and pulsatility in pseudoxanthoma elasticum.
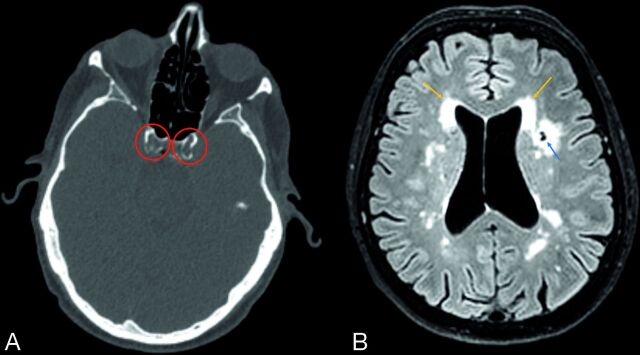
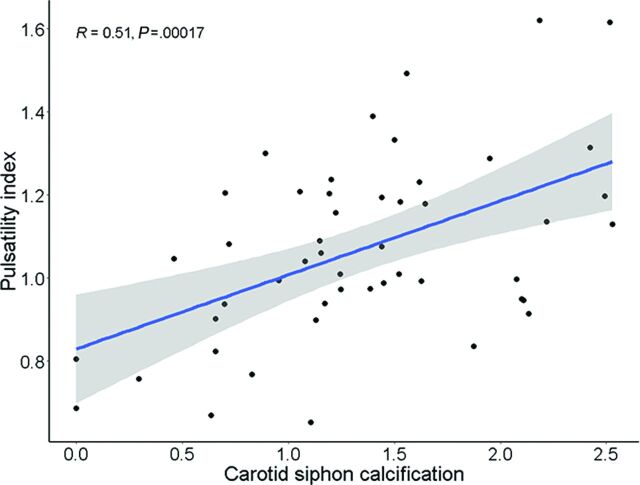
Materials and methods: Fifty patients with pseudoxanthoma elasticum and 40 age- and sex-matched controls underwent 3T MR imaging, including 2D phase-contrast acquisitions for flow pulsatility in the assessment of ICA and MCA and FLAIR acquisitions for brain volumes, white matter lesions, and infarctions. All patients with pseudoxanthoma elasticum underwent CT scanning to measure siphon calcification. Flow pulsatility (2D phase-contrast), brain volumes, white matter lesions, and infarctions (3D T1 and 3D T2 FLAIR) were compared between patients and controls. The association between siphon calcification and pulsatility in pseudoxanthoma elasticum was tested with linear regression models.
Results: Patients with pseudoxanthoma elasticum (mean age, 57 [SD, 12] years; 24 men) had significantly higher pulsatility indexes (1.05; range, 0.94-1.21 versus 0.94; range, 0.82-1.04; P = .02), lower mean GM volumes (597 [SD, 53] mL versus 632 [SD, 53] mL; P < .01), more white matter lesions (2.6; range, 0.5-7.5 versus 1.1; range, 0.5-2.4) mL; P = .05), and more lacunar infarctions (64 versus 8, P = .04) than controls (mean age, 58 [SD, 11] years; 20 men). Carotid siphon calcification was associated with higher pulsatility indexes in patients with pseudoxanthoma elasticum (β = 0.10; 95% CI, 0.01-0.18).
Conclusions: Patients with pseudoxanthoma elasticum have increased intracranial artery flow pulsatility and measures of small-vessel disease. Carotid siphon calcification might underlie the high prevalence of cerebrovascular disease in pseudoxanthoma elasticum.
© 2024 by American Journal of Neuroradiology.
Figures
Similar articles
-
Pulsatility Attenuation along the Carotid Siphon in Pseudoxanthoma Elasticum.AJNR Am J Neuroradiol. 2021 Nov;42(11):2030-2033. doi: 10.3174/ajnr.A7288. Epub 2021 Sep 24. AJNR Am J Neuroradiol. 2021. PMID: 34561212 Free PMC article.
-
Prevalence and severity of arterial calcifications in pseudoxanthoma elasticum (PXE) compared to hospital controls. Novel insights into the vascular phenotype of PXE.Atherosclerosis. 2017 Jan;256:7-14. doi: 10.1016/j.atherosclerosis.2016.11.012. Epub 2016 Nov 13. Atherosclerosis. 2017. PMID: 27940376
-
Is arterial stiffness in the carotid artery associated with choroidal thinning in patients with pseudoxanthoma elasticum or controls?Acta Ophthalmol. 2020 Aug;98(5):492-499. doi: 10.1111/aos.14346. Epub 2020 Jan 13. Acta Ophthalmol. 2020. PMID: 31943777
-
[Cerebrovascular disease and pseudoxanthoma elasticum: apropos of a case].Riv Neurol. 1981 Sep-Oct;51(5):261-73. Riv Neurol. 1981. PMID: 7031827 Review. Italian.
-
Pseudoxanthoma elasticum: a clinical, histopathological, and molecular update.Surv Ophthalmol. 2003 Jul-Aug;48(4):424-38. doi: 10.1016/s0039-6257(03)00053-5. Surv Ophthalmol. 2003. PMID: 12850230 Review.
Cited by
-
ABCC6 Involvement in Cerebral Small Vessel Disease: Potential Mechanisms and Associations.Genes (Basel). 2025 Jun 23;16(7):728. doi: 10.3390/genes16070728. Genes (Basel). 2025. PMID: 40725385 Free PMC article. Review.
-
Cyclical Etidronate Reduces the Progression of Arterial Calcifications in Patients with Pseudoxanthoma Elasticum: A 6-Year Prospective Observational Study.J Clin Med. 2024 Aug 7;13(16):4612. doi: 10.3390/jcm13164612. J Clin Med. 2024. PMID: 39200754 Free PMC article.
-
Tension at the gate: sensing mechanical forces at the blood-brain barrier in health and disease.J Neuroinflammation. 2024 Dec 18;21(1):325. doi: 10.1186/s12974-024-03321-2. J Neuroinflammation. 2024. PMID: 39696463 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous