

Assessment of Perfusion Volumes by a New Automated Software for Computed Tomography Perfusion
- PMID: 38548327
- PMCID: PMC11791637
- DOI: 10.1136/svn-2023-002964
Assessment of Perfusion Volumes by a New Automated Software for Computed Tomography Perfusion
Abstract
Introduction: To compare the perfusion volumes assessed by a new automated CT perfusion (CTP) software iStroke with the circular singular value decomposition software RAPID and determine its predictive value for functional outcome in patients with acute ischaemic stroke (AIS) who underwent endovascular treatment (EVT).
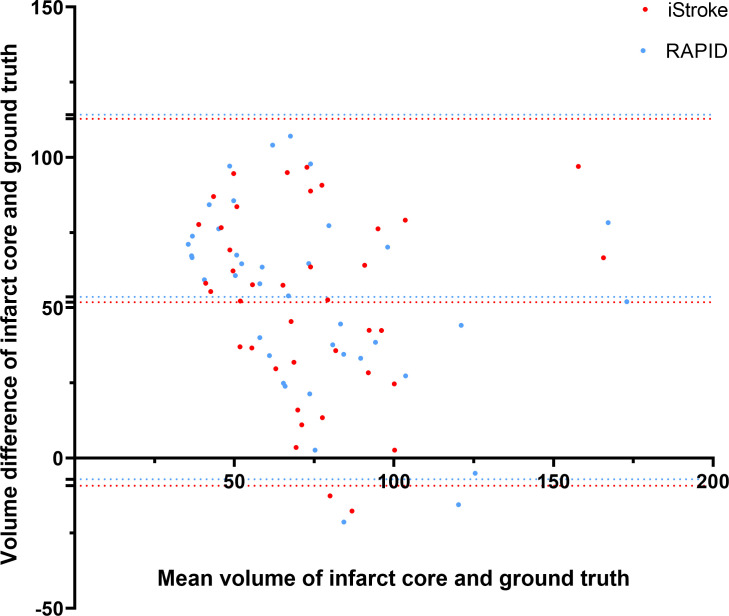
Methods: Data on patients with AIS were collected from four hospitals in China. All patients received CTP followed by EVT with complete recanalisation within 24 hours of symptom onset. We evaluated the agreement of CTP measures between the two softwares by Spearman's rank correlation tests and kappa tests. Bland-Altman plots were used to evaluate the agreement of infarct core volume (ICV) on CTP and ground truth on diffusion-weighted imaging (DWI). Logistic regression models were used to test the association between ICV on these two softwares and functional outcomes.
Results: Among 326 patients, 228 had DWI examinations and 40 of them had infarct volume >70 mL. In all patients, the infarct core and hypoperfusion volumes on iStroke had a strong correlation with those on RAPID (ρ=0.68 and 0.66, respectively). The agreement of large infarct core (volume >70 mL) was substantial (kappa=0.73, p<0.001) between these two softwares. The ICV measured by iStroke and RAPID was significantly correlated with independent functional outcome at 90 days (p=0.009 and p<0.001, respectively). In patients with DWI examinations and those with an ICV >70 mL, the ICV of iStroke and RAPID was comparable on individual agreement with ground truth.
Conclusion: The automatic CTP software iStroke is a reliable tool for assessing infarct core and mismatch volumes, making it clinically useful for selecting patients with AIS for acute reperfusion therapy in the extended time window.
Keywords: CT perfusion; Perfusion; Stroke; automated software; computed tomography perfusion; infarct core.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures

Similar articles
-
A New Automated Software for Enhanced Computed Tomography Perfusion Volume Assessment.World Neurosurg. 2025 Jul;199:124077. doi: 10.1016/j.wneu.2025.124077. Epub 2025 May 13. World Neurosurg. 2025. PMID: 40373966
-
Evaluation of Diffusion-Perfusion Mismatch in Acute Ischemic Stroke with a New Automated Perfusion-Weighted Imaging Software: A Retrospective Study.Neurol Ther. 2022 Dec;11(4):1777-1788. doi: 10.1007/s40120-022-00409-w. Epub 2022 Oct 6. Neurol Ther. 2022. PMID: 36201112 Free PMC article.
-
Agreement and Accuracy of Ischemic Core Volume Evaluated by Three CT Perfusion Software Packages in Acute Ischemic Stroke.J Stroke Cerebrovasc Dis. 2021 Aug;30(8):105872. doi: 10.1016/j.jstrokecerebrovasdis.2021.105872. Epub 2021 Jun 18. J Stroke Cerebrovasc Dis. 2021. PMID: 34153591
-
Endovascular thrombectomy vs best medical management for late presentation acute ischaemic stroke with large vessel occlusion without CT perfusion or MR imaging selection: A systematic review and meta-analysis.J Stroke Cerebrovasc Dis. 2024 Nov;33(11):108002. doi: 10.1016/j.jstrokecerebrovasdis.2024.108002. Epub 2024 Sep 7. J Stroke Cerebrovasc Dis. 2024. PMID: 39245396
-
Computed Tomography Perfusion in Acute Stroke Assessment.Cerebrovasc Dis. 2025;54(2):208-214. doi: 10.1159/000537729. Epub 2024 Mar 20. Cerebrovasc Dis. 2025. PMID: 38508150 Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical