

Evaluation of the risk of occupational exposure to antineoplastic drugs in healthcare sector: part II - the application of the FMECA method to compare manual vs automated preparation
- PMID: 38548384
- PMCID: PMC10978160
- DOI: 10.2478/aiht-2024-75-3803
Evaluation of the risk of occupational exposure to antineoplastic drugs in healthcare sector: part II - the application of the FMECA method to compare manual vs automated preparation
Abstract
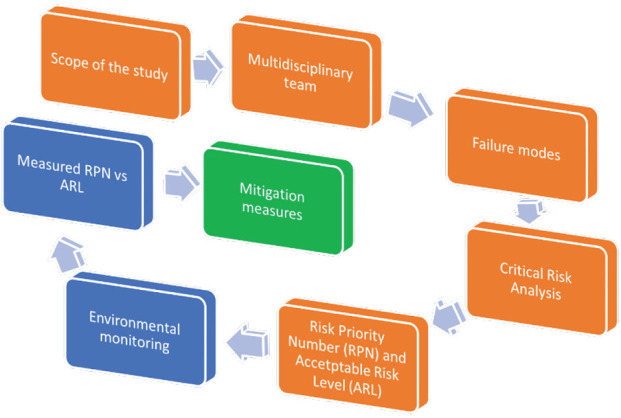
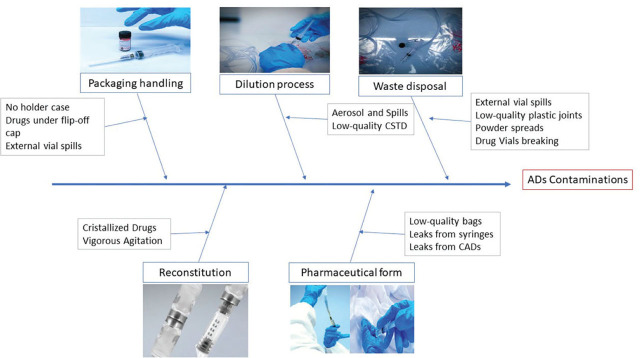
Healthcare workers handling antineoplastic drugs (ADs) in preparation units run the risk of occupational exposure to contaminated surfaces and associated mutagenic, teratogenic, and oncogenic effects of those drugs. To minimise this risk, automated compounding systems, mainly robots, have been replacing manual preparation of intravenous drugs for the last 20 years now, and their number is on the rise. To evaluate contamination risk and the quality of the working environment for healthcare workers preparing ADs, we applied the Failure Mode Effects and Criticality Analysis (FMECA) method to compare the acceptable risk level (ARL), based on the risk priority number (RPN) calculated from five identified failure modes, with the measured risk level (MRL). The model has shown higher risk of exposure with powdered ADs and containers not protected by external plastic shrink film, but we found no clear difference in contamination risk between manual and automated preparation. This approach could be useful to assess and prevent the risk of occupational exposure for healthcare workers coming from residual cytotoxic contamination both for current handling procedures and the newly designed ones. At the same time, contamination monitoring data can be used to keep track of the quality of working conditions by comparing the observed risk profiles with the proposed ARL. Our study has shown that automated preparation may have an upper hand in terms of safety but still leaves room for improvement, at least in our four hospitals.
Zdravstveni radnici koji rukuju antineoplastičnim lijekovima u posebnim jedinicama za njihovu pripremu izlažu se zagađenim površinama i riziku od s njima povezanim mutagenim, teratogenim i onkogenim učincima. Da bi se smanjio taj rizik, u posljednjih se 20-ak godina ručna priprema intravenskih lijekova sve više zamjenjuje automatiziranom. Da bismo ocijenili rizik od zagađenja i kakvoću radnog okoliša zdravstvenih radnika koji pripremaju antineoplastične lijekove, oslonili smo se na metodu analize mogućih pogrešaka u postupcima i kritičnosti njihovih posljedica (engl. failure mode effects and criticality analysis, krat. FMECA) radi usporedbe prihvatljive razine rizika (engl. acceptable risk level, krat. ARL), koja je zbroj ocjena prioriteta rizika (eng. risk priority number, krat. RPN) pet utvrđenih načina pogreške s izmjerenom razinom rizika (engl. measured risk level, krat. MRL). Taj nam je model pokazao da antineoplastični lijekovi u prahu i spremnicima koji nisu zaštićeni vanjskim plastičnim omotačem donose povećani rizik, ali nismo utvrdili dosljednu razliku u riziku od zagađenja između ručne i automatizirane pripreme. Ovaj pristup može biti koristan u procjeni i kontroli rizika od profesionalne izloženosti u zdravstvenih radnika rezidualnim citotoksičnim spojevima, bilo da se radi o postojećim ili tek planiranim/novoosmišljenim postupcima pripreme lijekova. Podatci dobiveni redovitim nadzorom (monitoringom) istodobno mogu poslužiti za praćenje kakvoće radnih uvjeta tako što će se usporediti s predviđenim profilom rizika koji je utvrđen ARL-om. Iako je naše istraživanje pokazalo da automatizirana priprema ima prednost nad ručnom u smislu sigurnosti, prostora za njezino poboljšanje ima podosta, naročito u našim četirima bolnicama koje su sudjelovale u istraživanju.
Keywords: acceptable risk levels; analiza pogrešaka i kritičnosti posljedica; failure mode effects and criticality analysis; izmjerene razine rizika; measured risk levels; ocjena prioriteta rizika; prihvatljive razine rizika; risk priority number.
© 2024 Stefano Dugheri et al., published by Sciendo.
Figures

Similar articles
-
Safety analysis of occupational exposure of healthcare workers to residual contaminations of cytotoxic drugs using FMECA security approach.Sci Total Environ. 2017 Dec 1;599-600:1939-1944. doi: 10.1016/j.scitotenv.2017.05.066. Epub 2017 May 23. Sci Total Environ. 2017. PMID: 28549369
-
Evaluation of the efficacy of additional measures introduced for the protection of healthcare personnel handling antineoplastic drugs.Ann Occup Hyg. 2013 Mar;57(2):240-50. doi: 10.1093/annhyg/mes057. Epub 2012 Aug 27. Ann Occup Hyg. 2013. PMID: 22926784
-
Association between occupational exposure levels of antineoplastic drugs and work environment in five hospitals in Japan.J Oncol Pharm Pract. 2011 Mar;17(1):29-38. doi: 10.1177/1078155210380485. Epub 2010 Aug 10. J Oncol Pharm Pract. 2011. PMID: 20699333
-
Environmental monitoring by surface sampling for cytotoxics: a review.Environ Monit Assess. 2017 Jan;189(2):52. doi: 10.1007/s10661-016-5762-9. Epub 2017 Jan 6. Environ Monit Assess. 2017. PMID: 28063118 Review.
-
Avoiding accidental exposure to intravenous cytotoxic drugs.Br J Nurs. 2014 Sep 11-24;23(16):S34, S36-9. doi: 10.12968/bjon.2014.23.Sup16.S34. Br J Nurs. 2014. PMID: 25203853 Review.
Cited by
-
A novel FMECA method for CNC machine tools based on D-GRA and data envelopment analysis.Sci Rep. 2024 Nov 4;14(1):26596. doi: 10.1038/s41598-024-77920-7. Sci Rep. 2024. PMID: 39496760 Free PMC article.
References
-
- Institute for Safe Medication Practices (ISIMP) ISMP list of high-alert medications in acute care settings [displayed 7 March 2024] Available at https://www.ismp.org/sites/default/files/attachments/2018-08/highAlert20....
-
- Carrez L, Falaschi L, Cingria L, Sadeghipour F, Bouchoud L, Bonnabry P. [Organisation et sécurisation du circuit des chimiothérapies: Exemple de la pharmacie des Hôpitaux Universitaires de Genève, in French] Pharmactuel. 2014;47:119–24.
-
- Palma E, Bufarini C. Robotized compounding of oncology drugs in a hospital pharmacy. Int J Pharm Compd. 2014;18:358–64. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical