

Management and outcome of patients with chronic myeloid leukemia in blast phase in the tyrosine kinase inhibitor era - analysis of the European LeukemiaNet Blast Phase Registry
- PMID: 38548962
- PMCID: PMC11073984
- DOI: 10.1038/s41375-024-02204-y
Management and outcome of patients with chronic myeloid leukemia in blast phase in the tyrosine kinase inhibitor era - analysis of the European LeukemiaNet Blast Phase Registry
Abstract
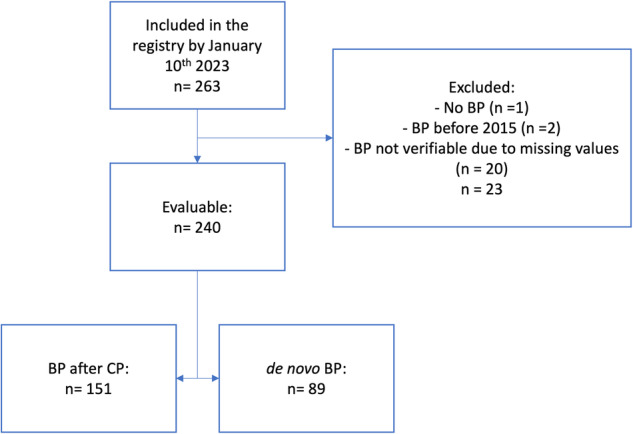
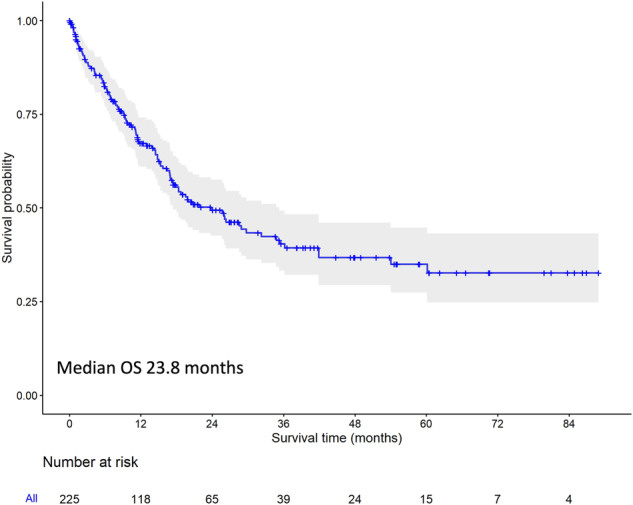
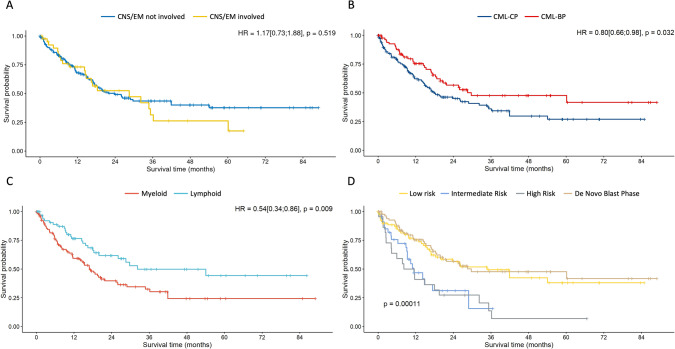
Blast phase (BP) of chronic myeloid leukemia (CML) still represents an unmet clinical need with a dismal prognosis. Due to the rarity of the condition and the heterogeneity of the biology and clinical presentation, prospective trials and concise treatment recommendations are lacking. Here we present the analysis of the European LeukemiaNet Blast Phase Registry, an international collection of the clinical presentation, treatment and outcome of blast phases which had been diagnosed in CML patients after 2015. Data reveal the expected heterogeneity of the entity, lacking a clear treatment standard. Outcomes remain dismal, with a median overall survival of 23.8 months (median follow up 27.8 months). Allogeneic stem cell transplantation (alloSCT) increases the rate of deep molecular responses. De novo BP and BP evolving from a previous CML do show slightly different features, suggesting a different biology between the two entities. Data show that outside clinical trials and in a real-world setting treatment of blast phase is individualized according to disease- and patient-related characteristics, with the aim of blast clearance prior to allogeneic stem cell transplantation. AlloSCT should be offered to all patients eligible for this procedure.
© 2024. The Author(s).
Conflict of interest statement
The registry received no support from pharmacological companies. The single authors have the following conflict of interest do declare: AB has participated in advisory boards from BMS, Janssen, GSK, Takeda and Sanofi and received honoraria and travel support from BMS, Janssen, GSK, Sanofi, Amgen, Gilead and Takeda; EL has received fees for lecturing and expert opinion from Novartis, Pfizer, Sotex, Pharmstandard and Fusion Pharma; HK supported lectures from Novartis and Angelini, travel support form Novartis; EM has received honoraria and travel support from Novartis, BMS and Pfizer; AG has participated in advisory boards from Roche and received honoraria and travel support form AMGEN, Novartis, Janssen, Pfizer; PE has received research support from Novartis and participated on advisory boards for Pfizer; DZ served as a member of advisory board for Novartis, served on a speakers bureau for Novartis, Pfizer and Angelini, as a consultant for Novartis and Angelini, and received travel support from Novartis, Pfizer, Angelini and Astra Zeneca; EPat has received consulting fees from KCR US, Inc., received honoraria from Amgen, Novartis, Servier, Angelini Pharma, Astellas Pharma and Pfizer and travel support from Amgen, Novartis, Servier, Angelini Pharma, Astellas Pharma, Pfizer, Jazz Pharma and BMS; KH has participated in advisory boards from Pfizer, Novartis, Incyte and GSK and received honoraria and travel support from Jazz, Novartis, Gilead, Roche, Pfizer, Amgen, Astellas Pharma, Merck and AbbVie; TE has received research support from Novartis, BMS, Incyte, Pfizer; GNF has participated in advisory boards from Novartis, received honoraria from BMS, Novartis, Gilead, Pfizer, Jazz Pharma, received travel support from Stemline, Gilead, Takeda and research support from Novartis; AK has participated in advisory boards and received honoraria and travel support from BMS/Celgene, Novartis and Pfizer; EF has received honoraria from Angelini, Novartis and Zentiva, is member of the Czech Advisory board for Novartis and has participated in advisory boards from Zentiva; LFC has participated in advisory boards from Novartis, BMS, Janssen, GSK, Astra Zeneca, Incyte, Beigene and Pfizer and received honoraria and travel support from BMS, Janssen, GSK, Astra Zeneca and Pfizer; KL has received honoraria for lectures, chairing sessions from Novartis, AbbVie, Angelini, Celgene, Pfizer, AOP Orphan and participated in advisory boards from Novartis, AbbVie, Angelini, Celgene, Pfizer, AOP Orphan; HH has participated in advisory boards and/or received travel support from BMS, Incyte, Novartis, Pfizer; SH has participated in advisory boards of Novartis, Celgene, BMS, AOP Orphan, AbbVie, and has received honoraria from Novartis, Celgene, BMS, AOP Orphan, AbbVie, Sanofi, Amgen; AH has received research support from Novartis, BMS, Incyte, Pfizer, Enliven and TERNS; ML has received research support from Novartis. All other authors declare no conflict of interest.
Figures
References
-
- Hochhaus A, Burchert A, Saussele S, Baerlocher GM, Mayer J, Brümmendorf TH, et al. Treatment free remission after nilotinib plus peg-interferon alpha induction and peg-interferon alpha maintenance therapy for newly diagnosed chronic myeloid leukemia patients; the tiger trial. Blood. 2023;142:446. doi: 10.1182/blood-2023-182792. - DOI - PubMed
-
- Saussele S, Richter J, Guilhot J, Gruber FX, Hjorth-Hansen H, Almeida A, et al. Discontinuation of tyrosine kinase inhibitor therapy in chronic myeloid leukaemia (EURO-SKI): a prespecified interim analysis of a prospective, multicentre, non-randomised, trial. Lancet Oncol. 2018;19:747–57. doi: 10.1016/S1470-2045(18)30192-X. - DOI - PubMed
-
- Hochhaus A, Masszi T, Giles FJ, Radich JP, Ross DM, Gómez Casares MT, et al. Treatment-free remission following frontline nilotinib in patients with chronic myeloid leukemia in chronic phase: results from the ENESTfreedom study. Leukemia. 2017;31:1525–31. doi: 10.1038/leu.2017.63. - DOI - PMC - PubMed
-
- Mahon F-X, Réa D, Guilhot J, Guilhot F, Huguet F, Nicolini F, et al. Discontinuation of imatinib in patients with chronic myeloid leukaemia who have maintained complete molecular remission for at least 2 years: the prospective, multicentre Stop Imatinib (STIM) trial. Lancet Oncol. 2010;11:1029–35. doi: 10.1016/S1470-2045(10)70233-3. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
