

Integration of a polygenic score into guideline-recommended prediction of cardiovascular disease
- PMID: 38551411
- PMCID: PMC11129792
- DOI: 10.1093/eurheartj/ehae048
Integration of a polygenic score into guideline-recommended prediction of cardiovascular disease
Abstract
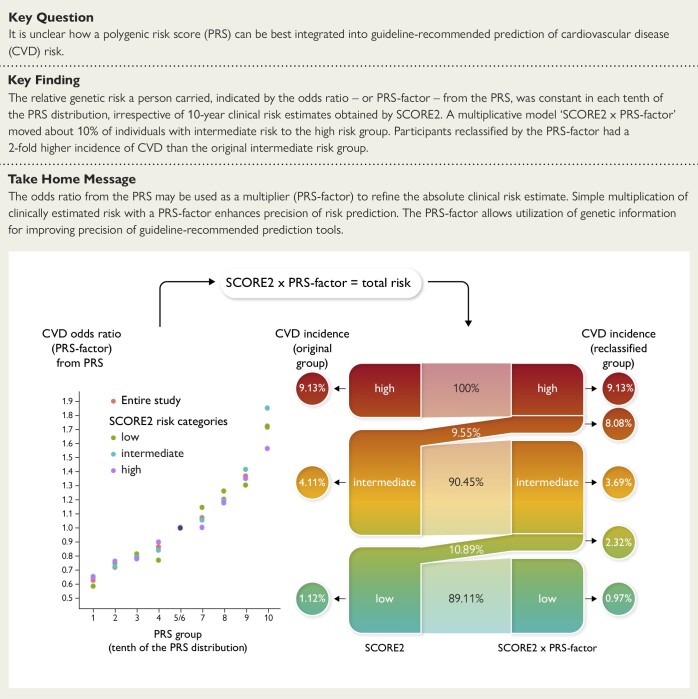
Background and aims: It is not clear how a polygenic risk score (PRS) can be best combined with guideline-recommended tools for cardiovascular disease (CVD) risk prediction, e.g. SCORE2.
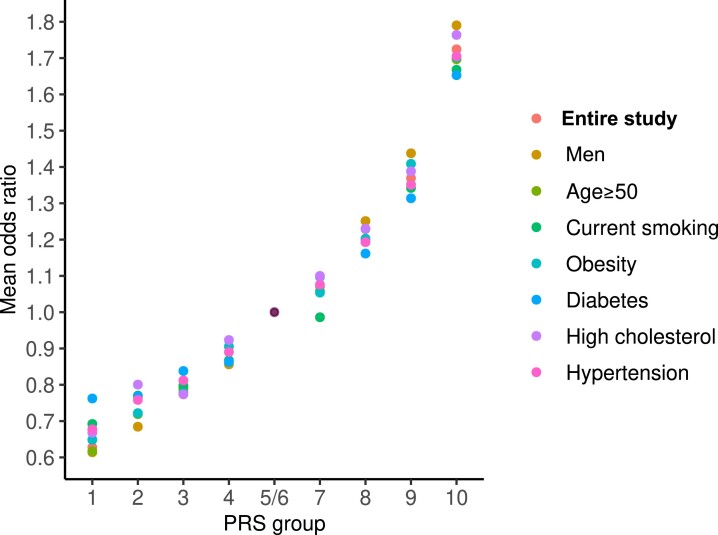
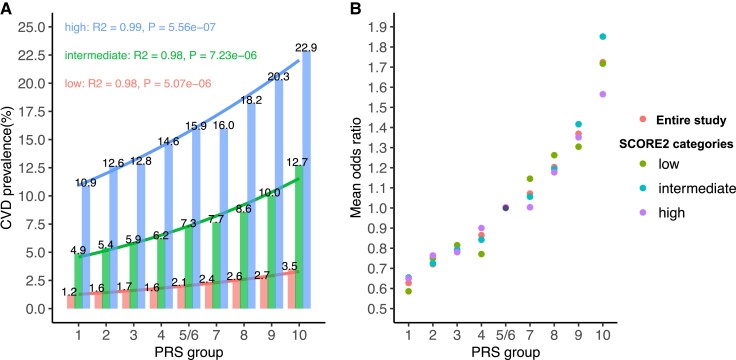
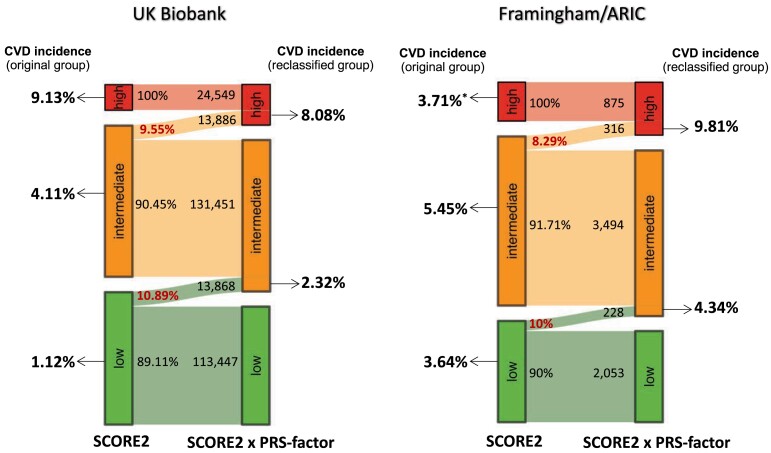
Methods: A PRS for coronary artery disease (CAD) was calculated in participants of UK Biobank (n = 432 981). Within each tenth of the PRS distribution, the odds ratios (ORs)-referred to as PRS-factor-for CVD (i.e. CAD or stroke) were compared between the entire population and subgroups representing the spectrum of clinical risk. Replication was performed in the combined Framingham/Atherosclerosis Risk in Communities (ARIC) populations (n = 10 757). The clinical suitability of a multiplicative model 'SCORE2 × PRS-factor' was tested by risk reclassification.
Results: In subgroups with highly different clinical risks, CVD ORs were stable within each PRS tenth. SCORE2 and PRS showed no significant interactive effects on CVD risk, which qualified them as multiplicative factors: SCORE2 × PRS-factor = total risk. In UK Biobank, the multiplicative model moved 9.55% of the intermediate (n = 145 337) to high-risk group increasing the individuals in this category by 56.6%. Incident CVD occurred in 8.08% of individuals reclassified by the PRS-factor from intermediate to high risk, which was about two-fold of those remained at intermediate risk (4.08%). Likewise, the PRS-factor shifted 8.29% of individuals from moderate to high risk in Framingham/ARIC.
Conclusions: This study demonstrates that absolute CVD risk, determined by a clinical risk score, and relative genetic risk, determined by a PRS, provide independent information. The two components may form a simple multiplicative model improving precision of guideline-recommended tools in predicting incident CVD.
Keywords: Cardiovascular disease; Polygenic risk score; Prevention guidelines; Primary prevention; Risk prediction; SCORE2.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Bäck M, et al. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice developed by the task force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies with the special contribution of the European Association of Preventive Cardiology (EAPC). Eur Heart J 2021;42:3227–337. 10.1093/eurheartj/ehab484 - DOI - PubMed
-
- Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019;140:e596–646. 10.1161/CIR.0000000000000678 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
