

Immunologic tumor microenvironment modulators for turning cold tumors hot
- PMID: 38551889
- PMCID: PMC11110955
- DOI: 10.1002/cac2.12539
Immunologic tumor microenvironment modulators for turning cold tumors hot
Abstract
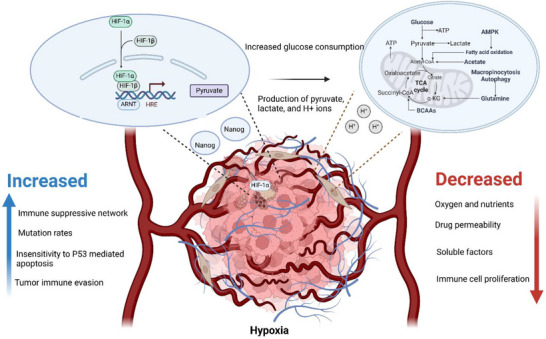
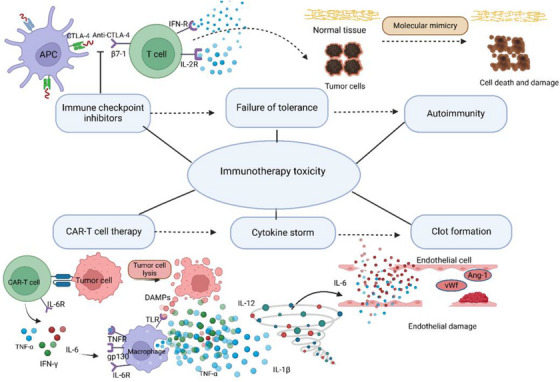
Tumors can be classified into distinct immunophenotypes based on the presence and arrangement of cytotoxic immune cells within the tumor microenvironment (TME). Hot tumors, characterized by heightened immune activity and responsiveness to immune checkpoint inhibitors (ICIs), stand in stark contrast to cold tumors, which lack immune infiltration and remain resistant to therapy. To overcome immune evasion mechanisms employed by tumor cells, novel immunologic modulators have emerged, particularly ICIs targeting cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) and programmed cell death protein 1/programmed death-ligand 1(PD-1/PD-L1). These agents disrupt inhibitory signals and reactivate the immune system, transforming cold tumors into hot ones and promoting effective antitumor responses. However, challenges persist, including primary resistance to immunotherapy, autoimmune side effects, and tumor response heterogeneity. Addressing these challenges requires innovative strategies, deeper mechanistic insights, and a combination of immune interventions to enhance the effectiveness of immunotherapies. In the landscape of cancer medicine, where immune cold tumors represent a formidable hurdle, understanding the TME and harnessing its potential to reprogram the immune response is paramount. This review sheds light on current advancements and future directions in the quest for more effective and safer cancer treatment strategies, offering hope for patients with immune-resistant tumors.
Keywords: cold tumor; hot tumor; immunologic modulator; immunotherapy; therapeutic strategy; tumor microenvironment.
© 2024 The Authors. Cancer Communications published by John Wiley & Sons Australia, Ltd on behalf of Sun Yat‐sen University Cancer Center.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Chen DS, Mellman I. Elements of cancer immunity and the cancer–immune set point. Nature. 2017;541(7637):321‐30. - PubMed
-
- Hegde PS, Karanikas V, Evers S. The where, the when, and the how of immune monitoring for cancer immunotherapies in the era of checkpoint inhibition. Clin Cancer Res. 2016;22(8):1865‐74. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
