

Cardiac Adverse Events and Remdesivir in Hospitalized Patients With COVID-19: A Post Hoc Safety Analysis of the Randomized DisCoVeRy Trial
- PMID: 38552208
- PMCID: PMC11327784
- DOI: 10.1093/cid/ciae170
Cardiac Adverse Events and Remdesivir in Hospitalized Patients With COVID-19: A Post Hoc Safety Analysis of the Randomized DisCoVeRy Trial
Abstract
Background: We aimed to evaluate the cardiac adverse events (AEs) in hospitalized patients with coronavirus disease 2019 (COVID-19) who received remdesivir plus standard of care (SoC) compared with SoC alone (control), as an association was noted in some cohort studies and disproportionality analyses of safety databases.
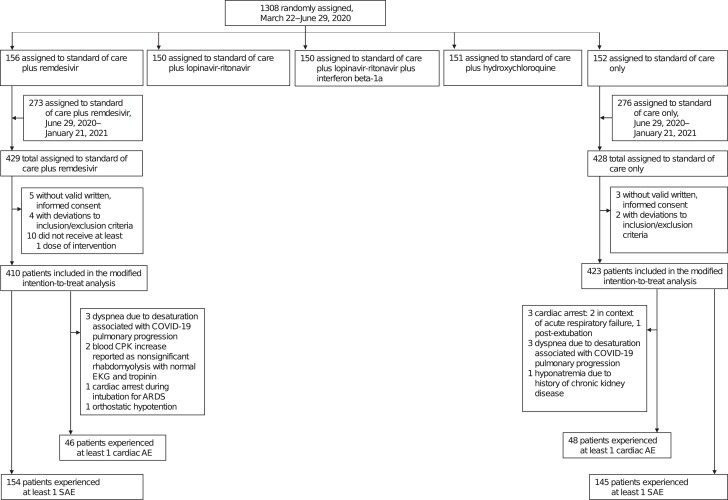
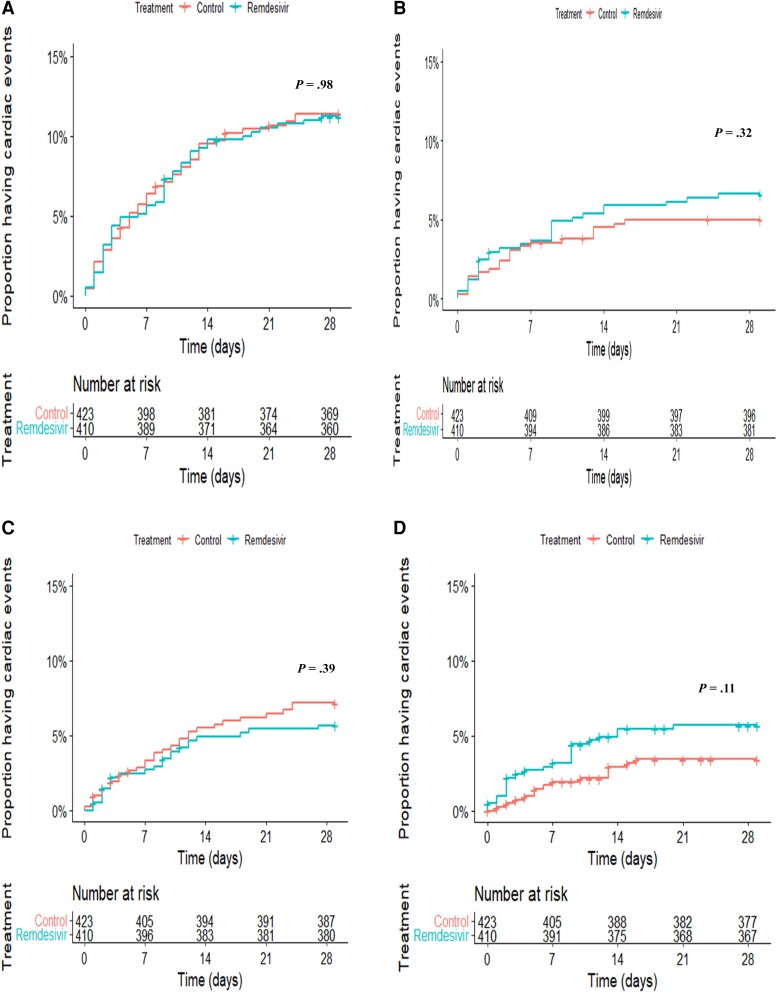
Methods: This post hoc safety analysis is based on data from the multicenter, randomized, open-label, controlled DisCoVeRy trial in hospitalized patients with COVID-19. Any first AE that occurred between randomization and day 29 in the modified intention-to-treat (mITT) population randomized to either remdesivir or control group was considered. Analysis was performed using Kaplan-Meier survival curves, and Kaplan-Meier estimates were calculated for event rates.
Results: Cardiac AEs were reported in 46 (11.2%) of 410 and 48 (11.3%) of 423 patients in the mITT population (n = 833) enrolled in the remdesivir and control groups, respectively. The difference between both groups was not significant (hazard ratio [HR], 1.0; 95% confidence interval [CI], .7-1.5; P = .98), even when serious and nonserious cardiac AEs were evaluated separately. The majority of reports in both groups were of arrhythmic nature (remdesivir, 84.8%; control, 83.3%) and were associated with a favorable outcome. There was no significant difference between the two groups in the occurrence of cardiac AE subclasses, including arrhythmic events (HR, 1.1; 95% CI, .7-1.7; P = .68).
Conclusions: Remdesivir treatment was not associated with an increased risk of cardiac AEs compared with control in patients hospitalized with moderate or severe COVID-19. These results are consistent with other randomized, controlled trials and meta-analyses. Clinical Trials Registration. NCT04315948; EudraCT 2020-000936-23.
Keywords: COVID-19; antiviral therapy; cardiac adverse events; randomized controlled trials; remdesivir.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. D. C. reports an human immunodeficiency virus grant from Janssen and lecture fees from Pfizer, outside the submitted work. F. M. reports grants and consulting fees from Pharmatheus, grants from Sanofi, and consulting fees from Ipsen, outside the submitted work. M. H. reports grants from the Belgian Center for Knowledge, the Fonds Erasme-COVID-Université Libre de Bruxelles, and the EU-Horizon programme, for the submitted work; support for attending meetings from Pfizer, MSD and Gilead, Pharmamar; support for participation on an advisory board for therapeutics on COVID-19 (DisCoVeRy trial); support for leadership for the Belgian guidelines on therapeutics for COVID-19; acting as president for the Belgian Society of Clinical Microbiology and Infectious Diseases; and payment for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Pfizer, Gilead, GKS, INSMED, and Shionogi. J. P. reports lecture fees from Gilead and MSD; support for attending meetings from Gilead, Eumedica, and Merck Sharp & Dohme, outside the submitted work. C. B. reports participation on a DSMB for 4Living Biotech and consulting fees from Da Volterra and Mylan Pharmaceuticals, outside the submitted work. R. G. reports consulting fees from Celgene, Novartis, Roche, Bristol Myers Squibb, Takeda, AbbVie, AstraZeneca, Janssen, Merck Sharp & Dohme, Merck, Gilead, and Daiichi Sankvo; lecture fees from Celgene, Roche, Merck, Takeda, AstraZeneca, Novartis, Amgen, Bristol Myers Squibb, Merck Sharp & Dohme, Sandoz, AbbVie, Gilead, and Daiichi Sankvo; support for attending meetings from Roche, Amgen, Janssen, AstraZeneca, Novartis, Merck Sharp & Dohme, Celgene, Gilead, Bristol Myers Squibb, AbbVie, and Daiichi Sankvo; participation on a DSMB for Celgene, Novartis, Roche, Bristol Myers Squibb, Takeda, AbbVie, AstraZeneca, Janssen, Merck Sharp & Dohme, Merck, Gilead, and Daiichi Sankyo; research grants from Celgene, Roche, Merck, Takeda, AstraZeneca, Novartis, Amgen, Bristol Myers Squibb, Merck Sharp & Dohme, Sandoz, AbbVie, Gilead, and Daiichi Sankyo; and stock or stock options from Novo Nordisk, Lilly. J.-A. P. reports consulting fees from Pfizer, Merck Sharp & Dohme, Janssen-Cilag, and AOP Orphan Pharmaceuticals; lecture fees from Cepheid, Pfizer, and Gilead; and support for attending meetings from Pfizer and Gilead. C. A. reports lecture fees from Insmed, GSK, Moderna, AstraZeneca, and Chiesi; grants or contracts from FEDER funding; support for attending meetings from Home perf; a leadership or fiduciary role as president of the Scientific Council of the French Respiratory Society; and serving as a member of the French ANRS-MIE for COVID and member of the COVID Group of the French Public Health High Council. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
Comment in
-
True DisCoVeRy of COVID-19 Disease Burden Versus Speculated Antiviral Cardiovascular Risk Requires a Control Group.Clin Infect Dis. 2024 Aug 16;79(2):392-394. doi: 10.1093/cid/ciae172. Clin Infect Dis. 2024. PMID: 38552189 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
