

Deconstructing pathological tau by biological process in early stages of Alzheimer disease: a method for quantifying tau spatial spread in neuroimaging
- PMID: 38552342
- PMCID: PMC10995809
- DOI: 10.1016/j.ebiom.2024.105080
Deconstructing pathological tau by biological process in early stages of Alzheimer disease: a method for quantifying tau spatial spread in neuroimaging
Abstract
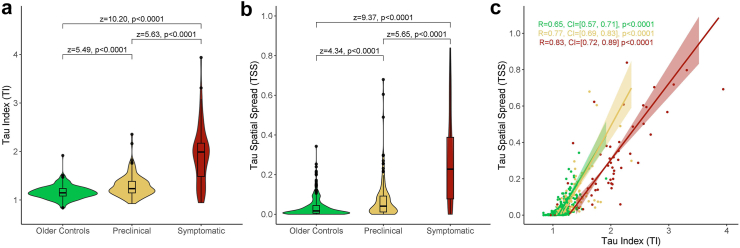
Background: Neuroimaging studies often quantify tau burden in standardized brain regions to assess Alzheimer disease (AD) progression. However, this method ignores another key biological process in which tau spreads to additional brain regions. We have developed a metric for calculating the extent tau pathology has spread throughout the brain and evaluate the relationship between this metric and tau burden across early stages of AD.
Methods: 445 cross-sectional participants (aged ≥ 50) who had MRI, amyloid PET, tau PET, and clinical testing were separated into disease-stage groups based on amyloid positivity and cognitive status (older cognitively normal control, preclinical AD, and symptomatic AD). Tau burden and tau spatial spread were calculated for all participants.
Findings: We found both tau metrics significantly elevated across increasing disease stages (p < 0.0001) and as a function of increasing amyloid burden for participants with preclinical (p < 0.0001, p = 0.0056) and symptomatic (p = 0.010, p = 0.0021) AD. An interaction was found between tau burden and tau spatial spread when predicting amyloid burden (p = 0.00013). Analyses of slope between tau metrics demonstrated more spread than burden in preclinical AD (β = 0.59), but then tau burden elevated relative to spread (β = 0.42) once participants had symptomatic AD, when the tau metrics became highly correlated (R = 0.83).
Interpretation: Tau burden and tau spatial spread are both strong biomarkers for early AD but provide unique information, particularly at the preclinical stage. Tau spatial spread may demonstrate earlier changes than tau burden which could have broad impact in clinical trial design.
Funding: This research was supported by the Knight Alzheimer Disease Research Center (Knight ADRC, NIH grants P30AG066444, P01AG026276, P01AG003991), Dominantly Inherited Alzheimer Network (DIAN, NIH grants U01AG042791, U19AG03243808, R01AG052550-01A1, R01AG05255003), and the Barnes-Jewish Hospital Foundation Willman Scholar Fund.
Keywords: Alzheimer disease; Positron emission tomography; Tau propagation; Tau spread.
Copyright © 2024. Published by Elsevier B.V.
Conflict of interest statement
Declaration of interests Data collection and sharing for this project was supported by the Dominantly Inherited Alzheimer Network (DIAN, U19-AG032438) funded by the National Institute on Aging (NIA), the Alzheimer's Association (SG-20-690363-DIAN), the German Center for Neurodegenerative Diseases (DZNE), the Queen Square Dementia Biomedical Research Centre and the Medical Research Council Dementias Platform UK (MR/L023784/1 and MR/009076/1). Partial support has also been provided by research and development grants for dementia from the Japan Agency for Medical Research and Development (JP22dk0207049), AMED, the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), Korea Dementia Research Center (KDRC) funded by the Ministry of Health & Welfare and Ministry of Science and ICT, Republic of Korea (HI21C0066), the Spanish Institute of Health Carlos III (ISCIII), the Canadian Institutes of Health Research (TAD-125697), the Canadian Consortium of Neurodegeneration and Aging, the Brain Canada Foundation, Fonds de Recherche du Québec, and the Raul Carrea Institute for Neurological Research (FLENI). In addition to the acknowledged funding sources for this research, the authors of this manuscript have received financial support from the National Institutes of Health (BMA, TLSB, JH, JCM, CX), National Institute on Aging (AJA, RJB, CC), National Institute of Neurological Disorders and Stroke (RJB), Alzheimer's Association (RJB, CC), DIAN-TU-001 Tau NextGen and OLE (RJB), Biogen (RJB), AbbVie (RJB), Bristol Myers Squibb (RJB), Novartis (RJB), Centene Corporation (RJB), Rainwater Foundation (RJB), Association for Frontotemporal Degeneration FTD Biomarkers Initiative (RJB), BrightFocus Foundation (RJB), Cure Alzheimer's Fund (RJB), Coins for Alzheimer's Research Trust Fund (RJB), Eisai (RJB), The Foundation for Barnes-Jewish Hospital (RJB), TargetALS (RJB), Good Ventures Foundation (RJB), DIAN-TU Pharma Consortium (RJB), Eli Lilly (RJB, TLSB), Avid Radiopharmaceuticals (TLSB), Hoffman-La Roche (RJB), CogState (RJB), Signant (RJB), Siemens (TLSB), and Michael J. Fox Foundation (CC). Travel support was received from Hoffman-La Roche (RJB), Alzheimer's Association Roundtable (RJB), Duke Margolis Alzheimer's Roundtable (RJB), BrightFocus Foundation (RJB), Tau Consortium Investigator's Meeting (RJB), Fondazione Prada (RJB), NAPA Advisory Council on Alzheimer's Research (RJB), and Somalogics (CC). Consultations have been declared for Biogen (TLSB), Eli Lilly (TLSB), Eisai (TLSB), Siemens (TLSB), Bristol Myers Squibb (TLSB), Alector (CC), Circular Genomics (CC), Parabon Nanolabs (JH), Hoffman-La Roche (JH), AlzPath (JH), Prothena (JH), Barcelona Brain Research Center (JCM), Native Alzheimer Disease-Related Resource Center in Minority Aging Research (JCM), and Diadem (CX). Honoraria was received from Korean Dementia Association (RJB), American Neurological Association (RJB), Fondazione Prada (RJB), Weill Cornell Medical College (RJB), Harvard University (RJB), Biogen (TLSB), Eisai (TLSB), Montefiore Grand Rounds NY (JCM), and Tetra-Inst ADRC seminar series Grand Rounds NY (JCM). Patents have been declared for NfL as a marker for ICANs due to CAR-T (BMA), methods for measuring the metabolism of CNS derived biomolecules in vivo (RJB), methods for measuring the metabolism of neutrally derived biomolecules in vivo (RJB), plasma based methods for detecting CNS amyloid disposition (RJB), plasma based methods for determining A-Beta amyloidosis (RJB), methods of treating based on site-specific tau phosphorylation (RJB), and tau kinetic measurements (RJB). Authors participated on advisory boards for VID (BMA), NNTC (BMA), Hoffman-La Roche/Genentech (RJB), Biogen (RJB), UK Dementia Research Institute at University College London (RJB), Stanford University (RJB), Next Generation Translational Proteomics for Alzheimer's and Related Dementias (RJB), C2N Diagnostics (RJB), Eisai (TLSB), Siemens (TLSB), Eli Lilly (TLSB), Bristol Myers Squibb (TLSB), NIH-sponsored external advisor grants (TLSB), NIA-sponsored Caring Bridge and Wall-E (JH), Cure Alzheimer's Fund Research Strategy Council (JCM), Indiana University LEADS Advisory Board (JCM), and FDA Advisory Committee on Imaging Medical Products (CX). Other declared interests include royalties with equity ownership from C2N Diagnostics (RJB), partnering and receiving stock from Circular Genomics (CC), and being the executive director of DIAN (AD). Participation in the ASNR Alzheimer's and ARIA Study Group, QIBA Amyloid PET Working Group, Alzheimer's Association Clinical Tau PET Work Group, and American College of Radiology/AlzNet Work Group (TLSB). Precursors for radiopharmaceuticals and technology transfer were received from Avid Radiopharmaceuticals/Eli Lilly, LMI, and Cerveau/Lantheus (TLSB). Drugs and services were received from Eisai, Janssen, and Hoffman- La Roche for the DIAN-TU Next Generation Trial and DIAN-TU Gantenerumab Open Label Extension (RJB). All other authors have nothing to disclose.
Figures



References
-
- Morris J.C., Storandt M., McKeel D.W., et al. Cerebral amyloid deposition and diffuse plaques in “normal” aging: evidence for presymptomatic and very mild Alzheimer’s disease. Neurology. 1996;46(3):707–719. - PubMed
-
- Hardy J.A., Higgins G.A. Alzheimer's disease: the amyloid cascade hypothesis. Science. 1992;256(5054):184–185. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
