

Quality of life endpoints in cancer cachexia clinical trials: Systematic review 3 of the cachexia endpoints series
- PMID: 38553255
- PMCID: PMC11154790
- DOI: 10.1002/jcsm.13453
Quality of life endpoints in cancer cachexia clinical trials: Systematic review 3 of the cachexia endpoints series
Abstract
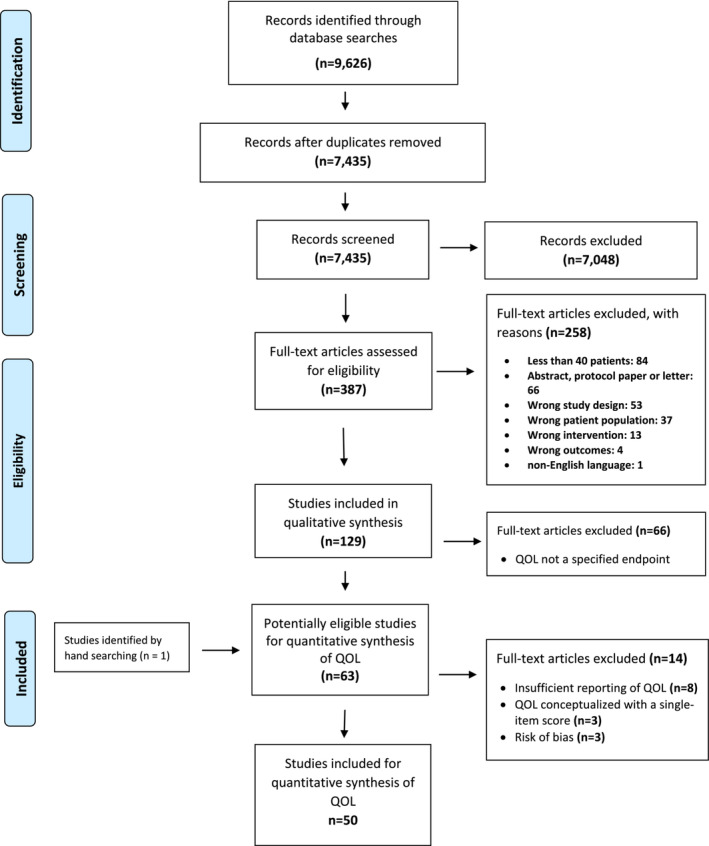
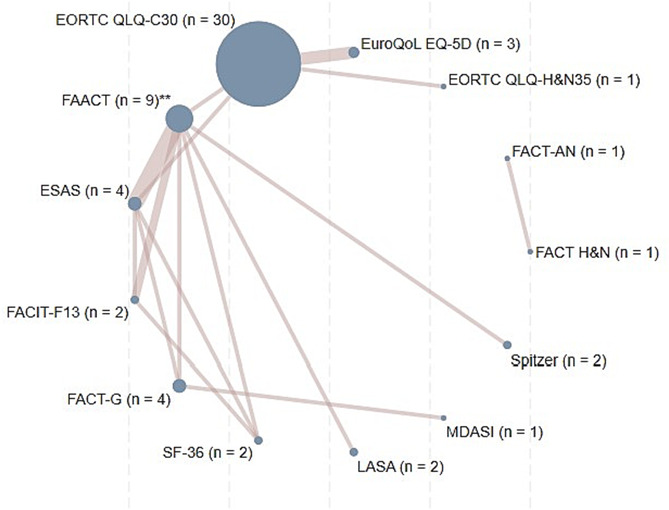
The use of patient-reported outcomes (PROMs) of quality of life (QOL) is common in cachexia trials. Patients' self-report on health, functioning, wellbeing, and perceptions of care, represent important measures of efficacy. This review describes the frequency, variety, and reporting of QOL endpoints used in cancer cachexia clinical trials. Electronic literature searches were performed in Medline, Embase, and Cochrane (1990-2023). Seven thousand four hundred thirty-five papers were retained for evaluation. Eligibility criteria included QOL as a study endpoint using validated measures, controlled design, adults (>18 years), ≥40 participants randomized, and intervention exceeding 2 weeks. The Covidence software was used for review procedures and data extractions. Four independent authors screened all records for consensus. Papers were screened by titles and abstracts, prior to full-text reading. PRISMA guidance for systematic reviews was followed. The protocol was prospectively registered via PROSPERO (CRD42022276710). Fifty papers focused on QOL. Twenty-four (48%) were double-blind randomized controlled trials. Sample sizes varied considerably (n = 42 to 469). Thirty-nine trials (78%) included multiple cancer types. Twenty-seven trials (54%) featured multimodal interventions with various drugs and dietary supplements, 11 (22%) used nutritional interventions alone and 12 (24%) used a single pharmacological intervention only. The median duration of the interventions was 12 weeks (4-96). The most frequent QOL measure was the EORTC QLQ-C30 (60%), followed by different FACIT questionnaires (34%). QOL was a primary, secondary, or exploratory endpoint in 15, 31 and 4 trials respectively, being the single primary in six. Statistically significant results on one or more QOL items favouring the intervention group were found in 18 trials. Eleven of these used a complete multidimensional measure. Adjustments for multiple testing when using multicomponent QOL measures were not reported. Nine trials (18%) defined a statistically or clinically significant difference for QOL, five with QOL as a primary outcome, and four with QOL as a secondary outcome. Correlation statistics with other study outcomes were rarely performed. PROMs including QOL are important endpoints in cachexia trials. We recommend using well-validated QOL measures, including cachexia-specific items such as weight history, appetite loss, and nutritional intake. Appropriate statistical methods with definitions of clinical significance, adjustment for multiple testing and few co-primary endpoints are encouraged, as is an understanding of how interventions may relate to changes in QOL endpoints. A strategic and scientific-based approach to PROM research in cachexia trials is warranted, to improve the research base in this field and avoid the use of QOL as supplementary measures.
Keywords: Cachexia; Cancer; Patient‐reported outcomes; Quality of life.
© 2024 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by Wiley Periodicals LLC.
Conflict of interest statement
Eric. J. Roeland has served as a member of the scientific advisory board for Napo Pharmaceuticals, Care4ward, Actimed Therapeutics, and Meter Health in the last 2 years, as a consultant for Veloxis Therapeutics, Aileron, and BYOMass, and as a member of the advisory board for Takeda. He has also served as a member on the data safety monitoring boards for Enzychem Lifesciences Pharmaceutical Company. Barry Laird has served as a member of the scientific advisory board for Actimed and Artelo. He has undertaken consultancy for Faraday, Kyona Kirin, and Grunenthal. Andrew S. J. Coats declares to have received honoraria and/or lecture fees from: Astra Zeneca, Bayer, Boehringer Ingelheim, Edwards, Eli Lilly, Menarini, Novartis, Servier, Vifor, Abbott, Actimed, Cardiac Dimensions, Corvia, CVRx, Enopace, ESN Cleer, Faraday, Impulse Dynamics, Respicardia, and Viatris. Richard Skipworth has received grant funding from Novartis, has been an advisory board member for Helsinn and Faraday Pharamaceuticals, and has provided consultancy work for Helsinn, Actimed Therapeutics, and Avidity Biosciences. Marianne J. Hjermstad, Gunnhild Jakobsen, Jann Arends, Trude R. Balstad, Leo R. Brown, Asta Bye, Olav F. Dajani, Ross D. Dolan, Marie T. Fallon, Christine Greil, Alexandra Grzyb, Stein Kaasa, Lisa Koteng, Anne M. May, James McDonald, Inger Ottestad, Iain Philips, Judith Sayers, Melanie R. Simpson, Tora S. Solheim, Mariana S. Sousa, Lisa H Koteng, and Ola M. Vagnildhaug declare that they have no conflict of interest.
Figures
References
-
- Fearon K, Strasser F, Anker SD, Bosaeus I, Bruera E, Fainsinger RL, et al. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol 2011;12:489–495. - PubMed
-
- Baracos VE. Cancer‐associated malnutrition. Eur J Clin Nutr 2018;72:1255–1259. - PubMed
-
- Wheelwright SJ, Darlington AS, Hopkinson JB, Fitzsimmons D, White A, Johnson CD. A systematic review to establish health‐related quality‐of‐life domains for intervention targets in cancer cachexia. BMJ Support Palliat Care 2016;6:307–314. - PubMed
-
- Karimi M, Brazier J. Health, health‐related quality of life, and quality of life: what is the difference? Pharmacoeconomics 2016;34:645–649. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
