

Tumor heterogeneity and clinically invisible micrometastases in metastatic breast cancer-a call for enhanced surveillance strategies
- PMID: 38553598
- PMCID: PMC10980766
- DOI: 10.1038/s41698-024-00572-3
Tumor heterogeneity and clinically invisible micrometastases in metastatic breast cancer-a call for enhanced surveillance strategies
Abstract
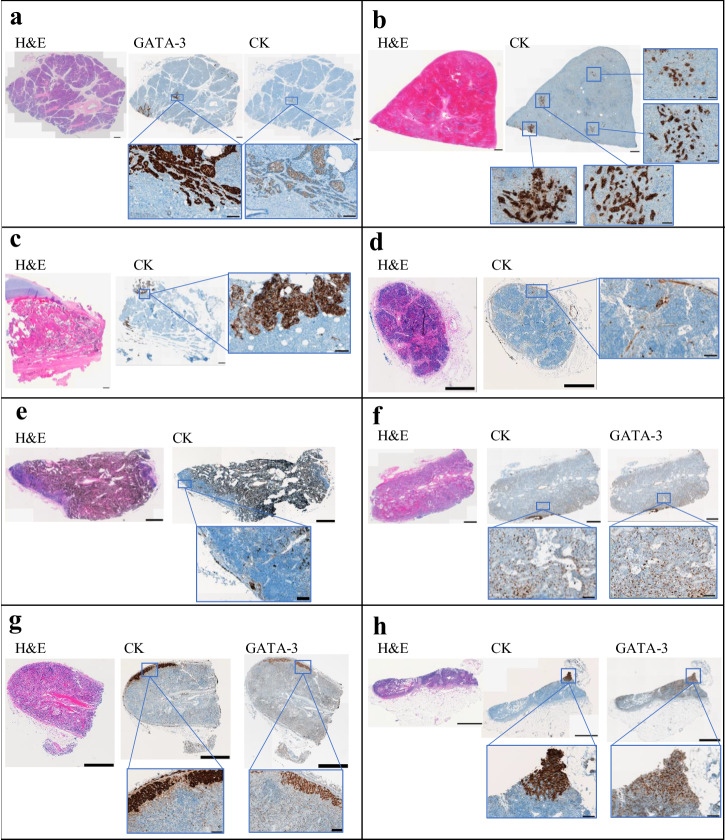
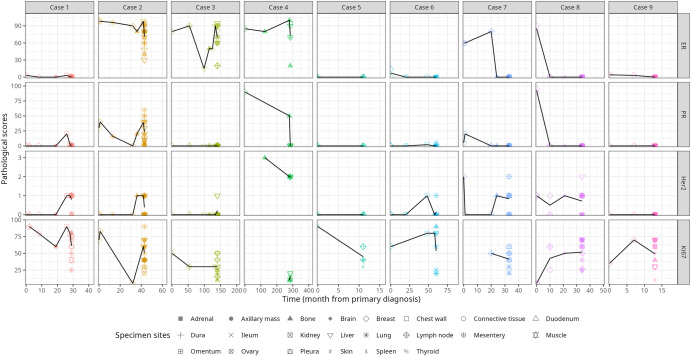
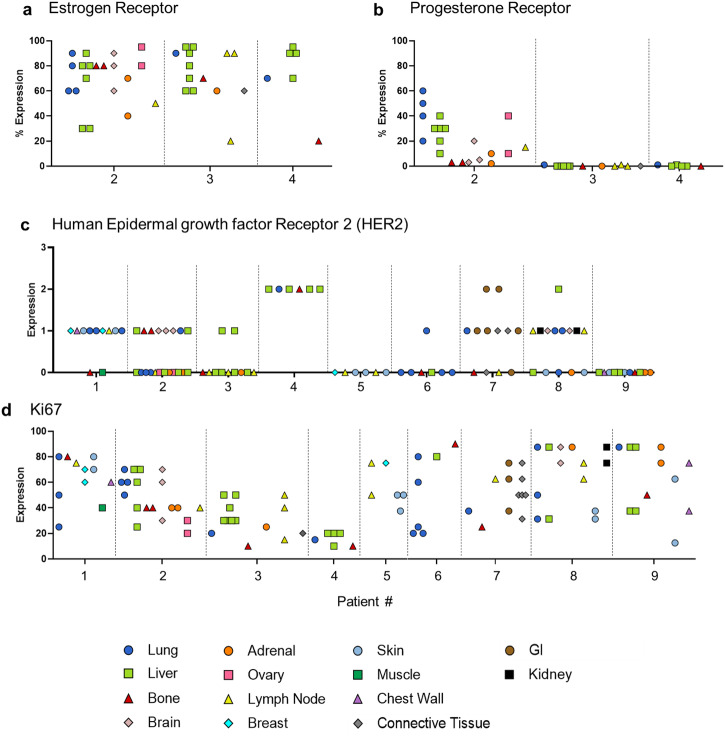
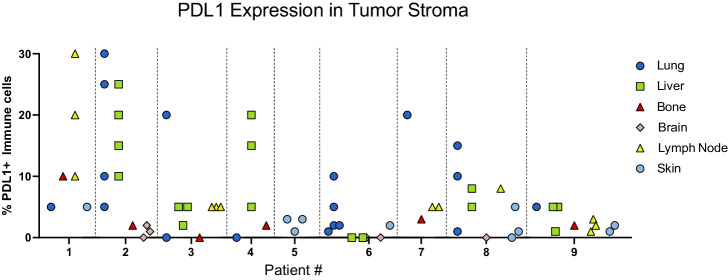
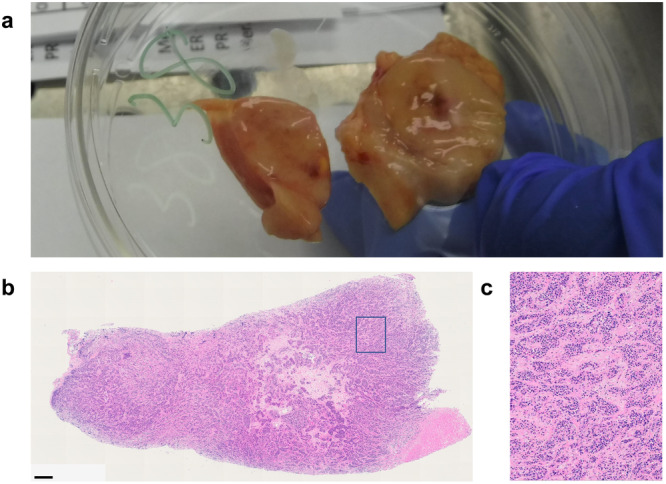
The biology of metastatic breast cancer (MBC) is understudied, primarily due to the difficulty of procuring multiple samples from patients with oligometastatic breast cancer. We developed a rapid postmortem tissue procurement program that allows the collection and analysis of numerous metastatic lesions, subclinical locations, and potential pre-metastatic niches that fall within this scope. We conducted a rapid postmortem tissue collection study on 9 patients with MBC. Patients and their families consented to donate tissues immediately after death in an IRB-approved study. Various disease subtypes, progression histories, organ involvement, and final causes of death are reported. In patients with hormone receptor-positive (HR+) disease, estrogen receptor (ER), progesterone receptor (PR), HER2, and Ki-67 expression were heterogeneous across metastatic lesions within individual patients. Disease phenotype at the end of life trended toward complete loss of HR expression. Nearly all (n = 7) patients exhibited extensive tumor involvement of additional organs that had not been previously diagnosed clinically and were not retrospectively visible on recent imaging. Of these seven individuals, three included organs uncommonly associated with MBC: kidney, spleen, pancreas, and ovary. Finally, we identified clinically undetectable micrometastases in several organs uncommonly involved in MBC. Our findings raise several clinically relevant questions regarding the mechanisms of metastatic progression. Insights from this study argue for better surveillance strategies for monitoring MBC. We highlight the need to capture more accurate biomarker information in the context of heterogeneous disease and urge the consideration of treatment strategies that combine multiple targeted therapies.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Bacon ER, Ihle K, Lee PP, Waisman JR. Building a rapid autopsy program – a step-by-step logistics guide. Transl. Med. Commun. 2020;5:23. doi: 10.1186/s41231-020-00074-x. - DOI
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
