

Personalizing non-small cell lung cancer treatment through patient-derived xenograft models: preclinical and clinical factors for consideration
- PMID: 38553659
- PMCID: PMC11333550
- DOI: 10.1007/s12094-024-03450-3
Personalizing non-small cell lung cancer treatment through patient-derived xenograft models: preclinical and clinical factors for consideration
Abstract
Purpose: In the pursuit of creating personalized and more effective treatment strategies for lung cancer patients, Patient-Derived Xenografts (PDXs) have been introduced as preclinical platforms that can recapitulate the specific patient's tumor in an in vivo model. We investigated how well PDX models can preserve the tumor's clinical and molecular characteristics across different generations.
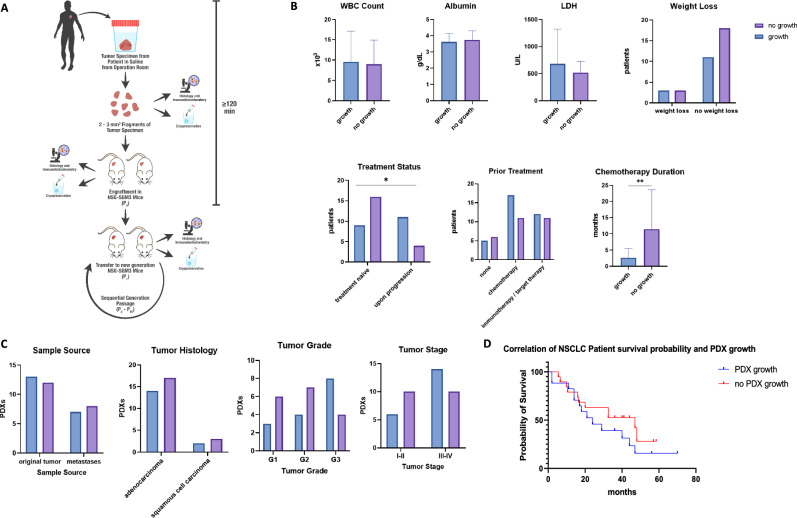
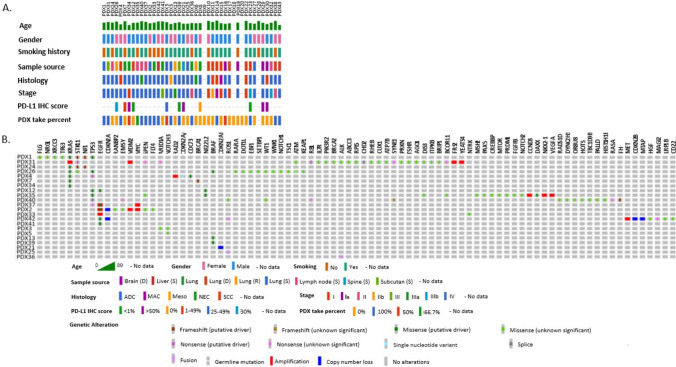
Methods: A Non-Small Cell Lung Cancer (NSCLC) PDX model was established in NSG-SGM3 mice and clinical and preclinical factors were assessed throughout subsequent passages. Our cohort consisted of 40 NSCLC patients, which were used to create 20 patient-specific PDX models in NSG-SGM3 mice. Histopathological staining and Whole Exome Sequencing (WES) analysis were preformed to understand tumor heterogeneity throughout serial passages.
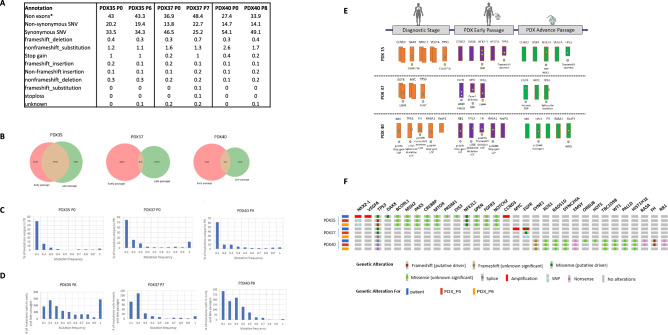
Results: The main factors that contributed to the growth of the engrafted PDX in mice were a higher grade or stage of disease, in contrast to the long duration of chemotherapy treatment, which was negatively correlated with PDX propagation. Successful PDX growth was also linked to poorer prognosis and overall survival, while growth pattern variability was affected by the tumor aggressiveness, primarily affecting the first passage. Pathology analysis showed preservation of the histological type and grade; however, WES analysis revealed genomic instability in advanced passages, leading to the inconsistencies in clinically relevant alterations between the PDXs and biopsies.
Conclusions: Our study highlights the impact of multiple clinical and preclinical factors on the engraftment success, growth kinetics, and tumor stability of patient-specific NSCLC PDXs, and underscores the importance of considering these factors when guiding and evaluating prolonged personalized treatment studies for NSCLC patients in these models, as well as signaling the imperative for additional investigations to determine the full clinical potential of this technique.
Keywords: NSG-SGM3; Non-small cell lung cancer; Patient-derived xenografts; Precision medicine; Preclinical models.
© 2024. The Author(s).
Conflict of interest statement
All authors declare no financial or non-financial competing interests.
Figures


Similar articles
-
Patient-derived non-small cell lung cancer xenograft mirrors complex tumor heterogeneity.Cancer Biol Med. 2021 Feb 15;18(1):184-198. doi: 10.20892/j.issn.2095-3941.2020.0012. Cancer Biol Med. 2021. PMID: 33628593 Free PMC article.
-
Patient-derived xenografts from non-small cell lung cancer brain metastases are valuable translational platforms for the development of personalized targeted therapy.Clin Cancer Res. 2015 Mar 1;21(5):1172-82. doi: 10.1158/1078-0432.CCR-14-1589. Epub 2014 Dec 30. Clin Cancer Res. 2015. PMID: 25549722
-
Utility of patient-derived xenografts to evaluate drug sensitivity and select optimal treatments for individual non-small-cell lung cancer patients.Mol Med. 2024 Nov 11;30(1):209. doi: 10.1186/s10020-024-00934-4. Mol Med. 2024. PMID: 39528952 Free PMC article.
-
Patient-derived xenografts of non small cell lung cancer: resurgence of an old model for investigation of modern concepts of tailored therapy and cancer stem cells.J Biomed Biotechnol. 2012;2012:568567. doi: 10.1155/2012/568567. Epub 2012 Apr 4. J Biomed Biotechnol. 2012. PMID: 22547927 Free PMC article. Review.
-
Patient-derived xenograft models for personalized medicine in colorectal cancer.Clin Exp Med. 2020 May;20(2):167-172. doi: 10.1007/s10238-020-00609-4. Epub 2020 Feb 25. Clin Exp Med. 2020. PMID: 32100151 Review.
Cited by
-
Personalized drug screening of patient-derived tumor-like cell clusters based on specimens obtained from percutaneous transthoracic needle biopsy in patients with lung malignancy: a real-world study.BMC Cancer. 2025 Apr 9;25(1):649. doi: 10.1186/s12885-025-14069-0. BMC Cancer. 2025. PMID: 40205326 Free PMC article.
References
-
- Wang M, Herbst RS, Boshoff C. Toward personalized treatment approaches for non-small-cell lung cancer. Nat Med 2021 278. 2021;27(8):1345–56. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
