

Sex Differences in Healthcare Utilization in Persons Living with Dementia Between 2000 and 2017: A Population-Based Study in Quebec, Canada
- PMID: 38554023
- PMCID: PMC11829507
- DOI: 10.1177/08982643241242512
Sex Differences in Healthcare Utilization in Persons Living with Dementia Between 2000 and 2017: A Population-Based Study in Quebec, Canada
Abstract
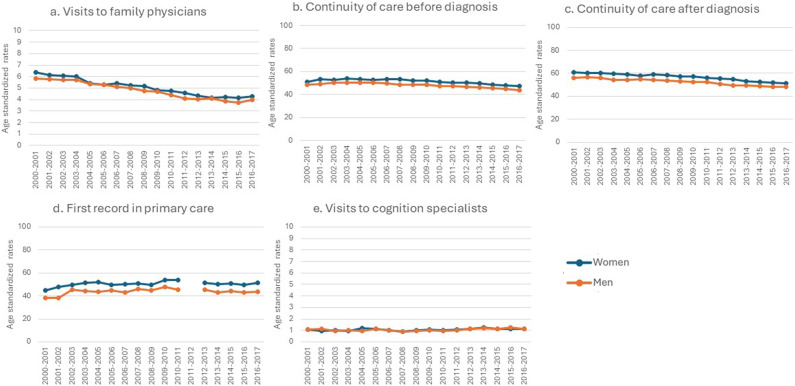
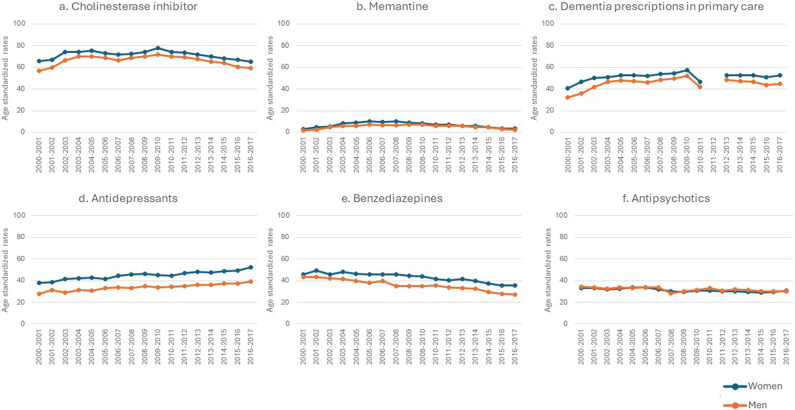
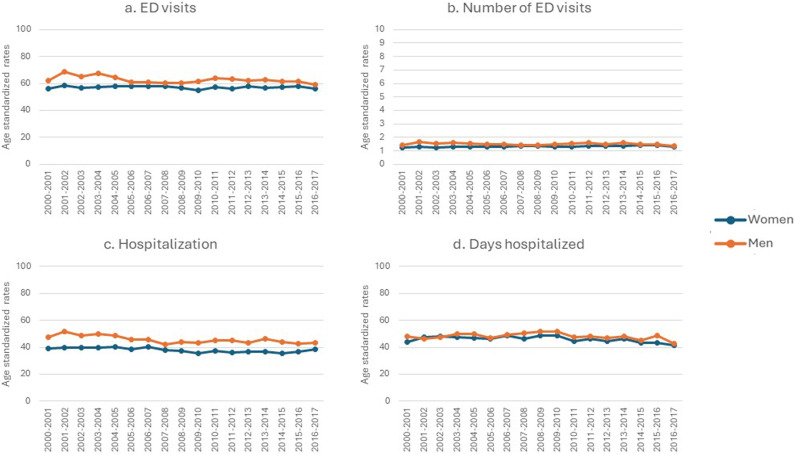
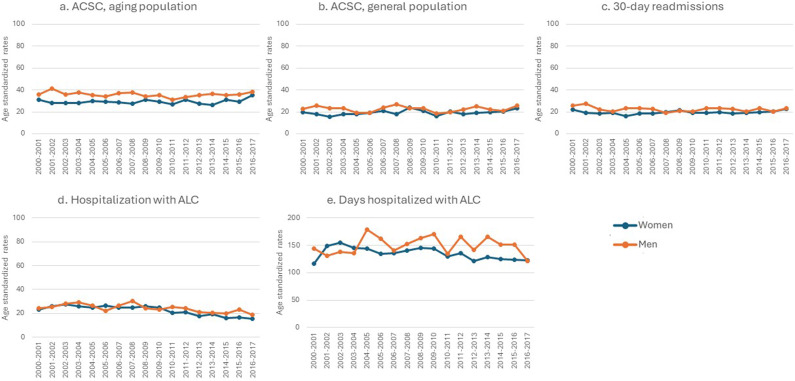
Objectives: Describe sex differences in healthcare utilization and mortality in persons with new dementia in Quebec, Canada. Methods: We conducted a repeated cohort study from 2000 to 2017 using health administrative databases. Community-dwelling persons aged 65+ with a new diagnosis of dementia were included. We measured 23 indicators of healthcare use across five care settings: ambulatory care, pharmacological care, acute hospital care, long-term care, and mortality. Clinically meaningful sex differences in age-standardized rates were determined graphically through expert consultations. Results: Women with dementia had higher rates of ambulatory care and pharmacological care, while men with dementia had higher acute hospital care, admission to long-term care, and mortality. There was no meaningful difference in visits to cognition specialists, antipsychotic prescriptions, and hospital death. Discussion: Men and women with dementia demonstrate differences in healthcare utilization and mortality. Addressing these differences will inform decision-makers, care providers and researchers and guide more equitable policy and interventions in dementia care.
Keywords: equity; health policy; healthcare utilization; persons with dementia; sex.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

References
-
- Ahmad O. B., Boschi-Pinto C., Lopez A. D., Murray C. J., Lozano R., Inoue M. (2001). Age standardization of rates: A new WHO standard. World Health Organization, 9(10), 1–14. https://www.academia.edu/download/31226140/3_WHO_pop_standard.pdf
-
- Alzheimer's Association . (nd). Women and Alzheimer's. https://www.alz.org/alzheimers-dementia/what-is-alzheimers/women-and-alz...
-
- Alzheimer Society Canada . (2017). Person-centred language guidelines. https://alzheimer.ca/sites/default/files/documents/Person-centred-langua...
-
- Alzheimer's Research UK . (2022). The impact of dementia on women. https://www.dementiaresearcher.nihr.ac.uk/the-impact-of-dementia-on-women/
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
