

Interventional treatment of refractory non-traumatic chylous effusions in patients with lymphoproliferative disorders
- PMID: 38554229
- PMCID: PMC10981590
- DOI: 10.1007/s10238-024-01312-4
Interventional treatment of refractory non-traumatic chylous effusions in patients with lymphoproliferative disorders
Abstract
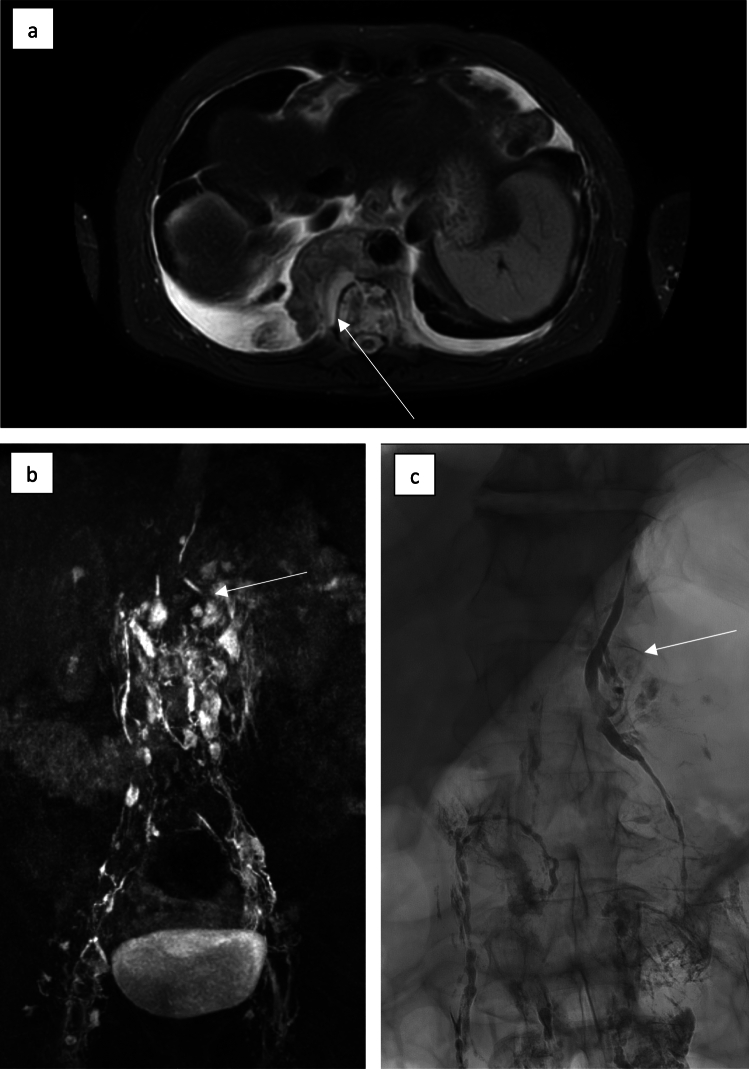
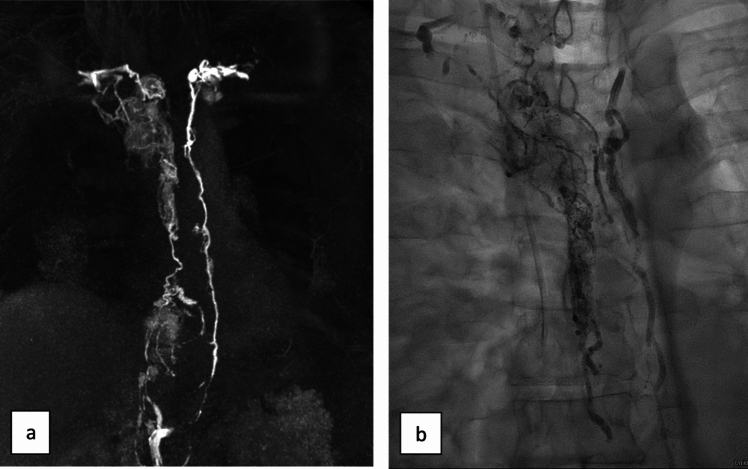
To report results of interventional treatment of refractory non-traumatic abdomino-thoracic chylous effusions in patients with lymphoproliferative disorders. 17 patients (10 male; mean age 66.7 years) with lymphoproliferative disorders suffered from non-traumatic chylous effusions (chylothorax n = 11, chylous ascites n = 3, combined abdomino-thoracic effusion n = 3) refractory to chemotherapy and conservative therapy. All underwent x-ray lymphangiography with iodized-oil to evaluate for and at the same time treat lymphatic abnormalities (leakage, chylo-lymphatic reflux with/without obstruction of central drainage). In patients with identifiable active leakage additional lymph-vessel embolization was performed. Resolution of effusions was deemed as clinical success. Lymphangiography showed reflux in 8/17 (47%), leakage in 2/17 (11.8%), combined leakage and reflux in 3/17 (17.6%), lymphatic obstruction in 2/17 (11.8%) and normal findings in 2/17 cases (11.8%). 12/17 patients (70.6%) were treated by lymphangiography alone; 5/17 (29.4%) with leakage received additional embolization (all technically successful). Effusions resolved in 15/17 cases (88.2%); 10/12 (83.3%) resolved after lymphangiography alone and in 5/5 patients (100%) after embolization. Time-to-resolution of leakage was significantly shorter after embolization (within one day in all cases) than lymphangiography (median 9 [range 4-30] days; p = 0.001). There was no recurrence of symptoms or post-interventional complications during follow-up (median 445 [40-1555] days). Interventional-radiological treatment of refractory, non-traumatic lymphoma-induced chylous effusions is safe and effective. Lymphangiography identifies lymphatic abnormalities in the majority of patients and leads to resolution of effusions in > 80% of cases. Active leakage is found in only a third of patients and can be managed by additional embolization.
Keywords: Chylothorax; Chylous ascites; Embolization; Lymphangiography; Lymphoproliferative disorders.
© 2024. The Author(s).
Conflict of interest statement
There are no financial arrangements that could be regarded as a conflict of interest in connection with the present work. Financial connections outside the present work: JAL: Speakers Bureau: Philips Healthcare (Netherlands), Bayer Vital (Germany); UIA: Speakers Bureau: Siemens Healthineers (Erlangen, Germany), CCP: Speakers Bureau: Philips Healthcare (Best, Netherlands), Bayer Vital (Germany), Guerbet (France), Julius Zorn GmbH (Germany).
Figures
References
-
- Fukumoto A, Terao T, Kuzume A, Tabata R, Tsushima T, Miura D, Ikeda D, Kamura Y, Narita K, Takeuchi M, Matsue K. Management of lymphoma-associated chylothorax by interventional radiology and chemotherapy: a report of five cases. Int J Hematol. 2022;116:579–85. 10.1007/s12185-022-03397-7. - PubMed
-
- Staats BA, Ellefson RD, Budahn LL, Dines DE, Prakash UB, Offord K. The lipoprotein profile of chylous and nonchylous pleural effusions. Mayo Clin Proc. 1980;55:700–4. - PubMed
-
- Pieper CC, Hur S, Sommer CM, Nadolski G, Maleux G, Kim J, Itkin M. Back to the future: lipiodol in lymphography-from diagnostics to theranostics. Invest Radiol. 2019;54:600–15. 10.1097/RLI.0000000000000578. - PubMed
-
- Pieper CC. Back to the future II-a comprehensive update on the rapidly evolving field of lymphatic imaging and interventions. Invest Radiol. 2023;58:610–40. 10.1097/RLI.0000000000000966. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
