

Genetic contribution to disease-course severity and progression in the SUPER-Finland study, a cohort of 10,403 individuals with psychotic disorders
- PMID: 38556557
- PMCID: PMC11420086
- DOI: 10.1038/s41380-024-02516-6
Genetic contribution to disease-course severity and progression in the SUPER-Finland study, a cohort of 10,403 individuals with psychotic disorders
Abstract
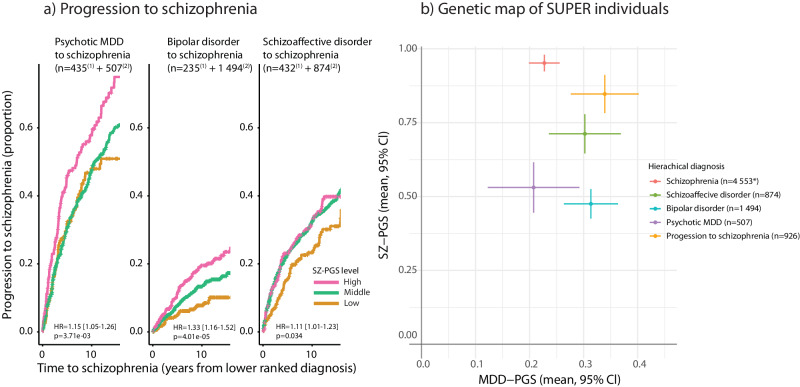
Genetic factors contribute to the susceptibility of psychotic disorders, but less is known how they affect psychotic disease-course development. Utilizing polygenic scores (PGSs) in combination with longitudinal healthcare data with decades of follow-up we investigated the contributing genetics to psychotic disease-course severity and diagnostic shifts in the SUPER-Finland study, encompassing 10 403 genotyped individuals with a psychotic disorder. To longitudinally track the study participants' past disease-course severity, we created a psychiatric hospitalization burden metric using the full-coverage and nation-wide Finnish in-hospital registry (data from 1969 and onwards). Using a hierarchical model, ranking the psychotic diagnoses according to clinical severity, we show that high schizophrenia PGS (SZ-PGS) was associated with progression from lower ranked psychotic disorders to schizophrenia (OR = 1.32 [1.23-1.43], p = 1.26e-12). This development manifested already at psychotic illness onset as a higher psychiatric hospitalization burden, the proxy for disease-course severity. In schizophrenia (n = 5 479), both a high SZ-PGS and a low educational attainment PGS (EA-PGS) were associated with increased psychiatric hospitalization burden (p = 1.00e-04 and p = 4.53e-10). The SZ-PGS and the EA-PGS associated with distinct patterns of hospital usage. In individuals with high SZ-PGS, the increased hospitalization burden was composed of longer individual hospital stays, while low EA-PGS associated with shorter but more frequent hospital visits. The negative effect of a low EA-PGS was found to be partly mediated via substance use disorder, a major risk factor for hospitalizations. In conclusion, we show that high SZ-PGS and low EA-PGS both impacted psychotic disease-course development negatively but resulted in different disease-course trajectories.
© 2024. The Author(s).
Conflict of interest statement
AO is a shareholder and employee of Abomics, a company offering pharmacogenetics-related ICT-solutions and consultation services. MD is a member of the Pfizer Finland FinnGen Advisory Board and a founder of Maze Therapeutics.
Figures



Similar articles
-
Schizophrenia polygenic risk score and 20-year course of illness in psychotic disorders.Transl Psychiatry. 2019 Nov 14;9(1):300. doi: 10.1038/s41398-019-0612-5. Transl Psychiatry. 2019. PMID: 31727878 Free PMC article.
-
Shared vulnerability and sex-dependent polygenic burden in psychotic disorders.Eur Neuropsychopharmacol. 2024 Sep;86:49-54. doi: 10.1016/j.euroneuro.2024.04.017. Epub 2024 Jun 27. Eur Neuropsychopharmacol. 2024. PMID: 38941950
-
Association of neurotransmitter pathway polygenic risk with specific symptom profiles in psychosis.Mol Psychiatry. 2024 Aug;29(8):2389-2398. doi: 10.1038/s41380-024-02457-0. Epub 2024 Mar 15. Mol Psychiatry. 2024. PMID: 38491343 Free PMC article.
-
Sleep and schizophrenia polygenic scores in non-affective and affective psychotic disorders.Psychol Med. 2025 Apr 15;55:e117. doi: 10.1017/S0033291725000844. Psychol Med. 2025. PMID: 40230302 Free PMC article.
-
Research Review: A guide to computing and implementing polygenic scores in developmental research.J Child Psychol Psychiatry. 2022 Oct;63(10):1111-1124. doi: 10.1111/jcpp.13611. Epub 2022 Mar 30. J Child Psychol Psychiatry. 2022. PMID: 35354222 Free PMC article. Review.
Cited by
-
Polygenic Scores for Schizophrenia and Educational Attainment Predict Global Functioning Across Psychiatric Hospitalization Among People with Schizophrenia.medRxiv [Preprint]. 2025 May 21:2025.05.20.25328039. doi: 10.1101/2025.05.20.25328039. medRxiv. 2025. PMID: 40661280 Free PMC article. Preprint.
-
General medical comorbidities in psychotic disorders in the Finnish SUPER study.Schizophrenia (Heidelb). 2024 Dec 31;10(1):124. doi: 10.1038/s41537-024-00546-1. Schizophrenia (Heidelb). 2024. PMID: 39741144 Free PMC article.
-
Profiles of Genetic Risks for Psychotic Disorders.JAMA Psychiatry. 2025 Sep 1;82(9):926-933. doi: 10.1001/jamapsychiatry.2025.1289. JAMA Psychiatry. 2025. PMID: 40632548
-
The outcome of major psychiatric and substance use disorders as an index of genetic risk and genetic heterogeneity.Psychol Med. 2025 Aug 14;55:e233. doi: 10.1017/S0033291725101116. Psychol Med. 2025. PMID: 40810310 Free PMC article.
References
-
- Hung YN, Yang SY, Kuo CJ, Lin SK. Diagnostic consistency and interchangeability of schizophrenic disorders and bipolar disorders: a 7-year follow-up study. Psychiatry Clin Neurosci. 2018;72:180–8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
