

Functional abilities, respiratory and cardiac function in a large cohort of adults with Duchenne muscular dystrophy treated with glucocorticoids
- PMID: 38556893
- PMCID: PMC11236054
- DOI: 10.1111/ene.16267
Functional abilities, respiratory and cardiac function in a large cohort of adults with Duchenne muscular dystrophy treated with glucocorticoids
Abstract
Background and purpose: The transition to adult services, and subsequent glucocorticoid management, is critical in adults with Duchenne muscular dystrophy. This study aims (1) to describe treatment, functional abilities, respiratory and cardiac status during transition to adulthood and adult stages; and (2) to explore the association between glucocorticoid treatment after loss of ambulation (LOA) and late-stage clinical outcomes.
Methods: This was a retrospective single-centre study on individuals with Duchenne muscular dystrophy (≥16 years old) between 1986 and 2022. Logistic regression, Cox proportional hazards models and survival analyses were conducted utilizing data from clinical records.
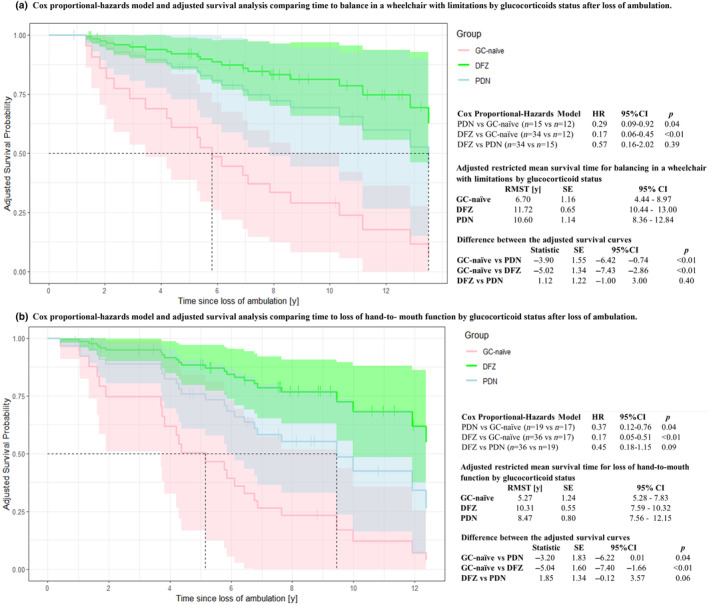
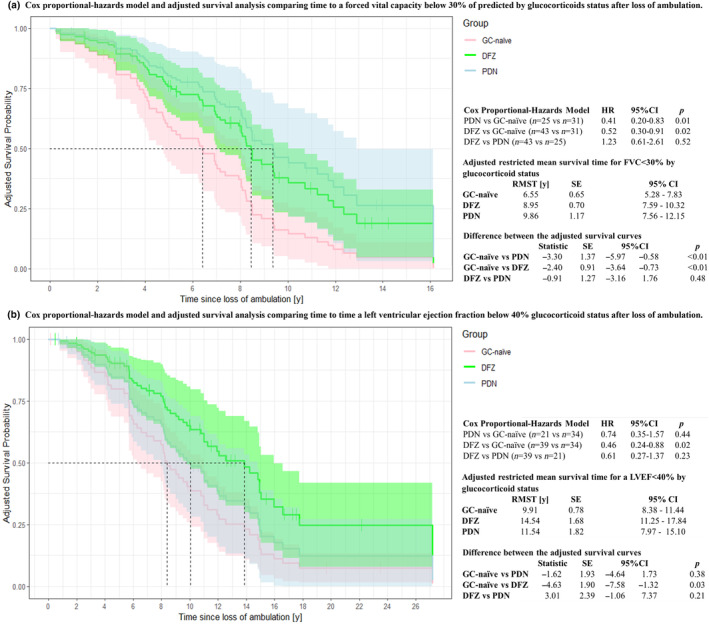
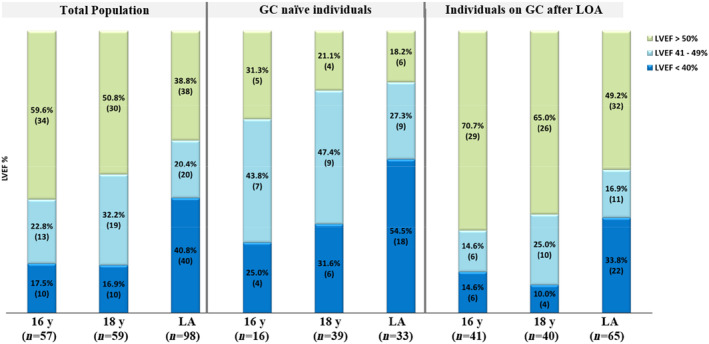
Results: In all, 112 individuals were included. Mean age was 23.4 ± 5.2 years and mean follow-up was 18.5 ± 5.5 years. At last assessment, 47.2% were on glucocorticoids; the mean dose of prednisone was 0.38 ± 0.13 mg/kg/day and of deflazacort 0.43 ± 0.16 mg/kg/day. At age 16 years, motor function limitations included using a manual wheelchair (89.7%), standing (87.9%), transferring from a wheelchair (86.2%) and turning in bed (53.4%); 77.5% had a peak cough flow <270 L/min, 53.3% a forced vital capacity percentage of predicted <50% and 40.3% a left ventricular ejection fraction <50%. Glucocorticoids after LOA reduced the risk and delayed the time to difficulties balancing in the wheelchair, loss of hand to mouth function, forced vital capacity percentage of predicted <30% and forced vital capacity <1 L and were associated with lower frequency of left ventricular ejection fraction <50%, without differences between prednisone and deflazacort. Glucocorticoid dose did not differ by functional, respiratory or cardiac status.
Conclusion: Glucocorticoids after LOA preserve late-stage functional abilities, respiratory and cardiac function. It is suggested using functional abilities, respiratory and cardiac status at transition stages for adult services planning.
Keywords: EK scale in adults with DMD; cardiac function in adults with DMD; glucocorticoid dose in adults with DMD; respiratory function in adults with DMD; transition to adulthood in DMD.
© 2024 The Authors. European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
M. Guglieri has been participating in advisory boards for PTC Therapeutics, Capricor, Pfizer and NS Pharma. She had research collaborations with ReveraGen, PTC, Sarepta, Duchenne UK and MDUK through Newcastle University. She is or has been Principal Investigator for clinical trials with Roche, Italfarmaco, Santhera, ReveraGen, Summit, Pfizer, PTC Therapeutics. She received speaker honoraria from Italfarmaco, Roche, Novartis and Sarepta. M. Schiava has received a grant by UK Duchenne through Newcastle University. C. Marini Bettolo has received a grant by Duchenne UK through Newcastle University. R. Muni‐Lofra has been participating in advisory boards for Biogen, Roche and Novartis and has delivered consultancy work for Pfizer, Italofarmaco, Sarepta, Summit and NS Pharma. AGM has served on medical/scientific advisory boards for Regenxbio, Sarepta, Biogen and Roche; and has received fees for consulting and training services for Biogen, Roche, Novartis, Biohaven, PTC, Sarepta, Italfarmaco, Dyne, Pfizer, Summit, Catabasis, Santhera, Vision, Lysogene, Modis, Amicus, Analysis Group, MDUK and DUK. The rest of the authors report no competing interests.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
