

This is a preprint.
Sex Bias in Prediction and Diagnosis of Cardiac Surgery Associated Acute Kidney Injury
- PMID: 38558997
- PMCID: PMC10980107
- DOI: 10.21203/rs.3.rs-3660617/v1
Sex Bias in Prediction and Diagnosis of Cardiac Surgery Associated Acute Kidney Injury
Update in
-
Sex bias in prediction and diagnosis of cardiac surgery associated acute kidney injury.BMC Nephrol. 2024 May 22;25(1):180. doi: 10.1186/s12882-024-03614-x. BMC Nephrol. 2024. PMID: 38778259 Free PMC article.
Abstract
Background: Female sex has been recognized as a risk factor for cardiac surgery associated acute kidney injury (CS-AKI). The current study sought to evaluate whether female sex is a risk factor for CS-AKI, or modifies the association of peri-operative change in serum creatinine with CS-AKI.
Methods: Observational study of adult patients undergoing cardiac surgery between 2000 and 2019 in a single U.S. center. The main variable of interest was registered patient sex, identified from electronic medical records. The main outcome was CS-AKI within 2 weeks of surgery.
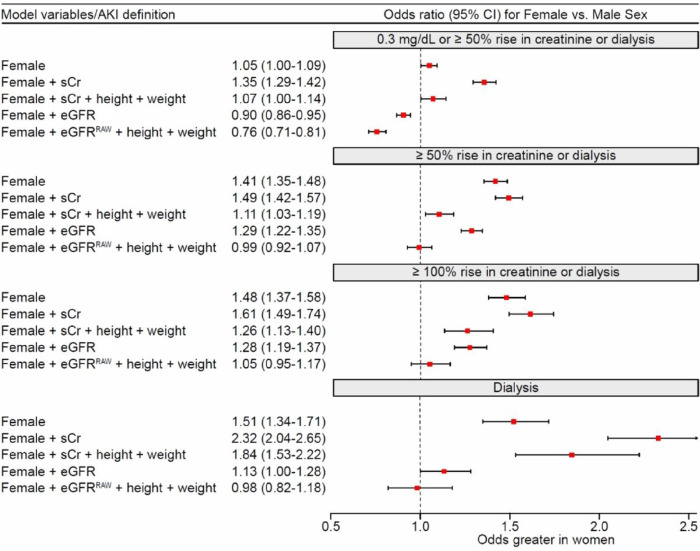
Results: Of 58526 patients, 19353 (33%) were female; 12934 (22%) incurred AKI based on ≥ 0.3 mg/dL or ≥ 50% rise in serum creatinine (any AKI), 3320 (5.7%) had moderate to severe AKI, and 1018 (1.7%) required dialysis within 2 weeks of surgery. Female sex was associated with higher risk for AKI in models that were based on preoperative serum creatinine (OR, 1.35; 95% CI, 1.29-1.42), and lower risk with the use of estimated glomerular filtration, (OR, 0.90; 95% CI, 0.86-0.95). The risk for moderate to severe CS-AKI for a given immediate peri-operative change in serum creatinine was higher in female compared to male patients (p < .0001 and p < .0001 for non-linearity), and the association was modified by pre-operative kidney function (p < .0001 for interaction).
Conclusions: The association of patient sex with CS-AKI and its direction was dependent on the operational definition of pre-operative kidney function, and differential outcome misclassification due to AKI defined by absolute change in serum creatinine.
Keywords: acute kidney injury; body surface area; cardiac surgery; estimated glomerular filtration rate; patient sex.
Conflict of interest statement
Conflict of interest disclosures: Dr. Demirjian and Cleveland Clinic Innovations Center hold U.S. Patent for predictive models for CS-AKI. Dr. Gillinov reports consultation services to Edwards, Medtronic, Artivion, Abbott, ClearFlow, and AtriCure. No other disclosures reported.
Figures



Similar articles
-
Sex bias in prediction and diagnosis of cardiac surgery associated acute kidney injury.BMC Nephrol. 2024 May 22;25(1):180. doi: 10.1186/s12882-024-03614-x. BMC Nephrol. 2024. PMID: 38778259 Free PMC article.
-
Clinical characteristics and risk factors of cardiac surgery associated-acute kidney injury progressed to chronic kidney disease in adults: A retrospective, observational cohort study.Front Cardiovasc Med. 2023 Mar 8;10:1108538. doi: 10.3389/fcvm.2023.1108538. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 36970343 Free PMC article.
-
Association between urinary dickkopf-3, acute kidney injury, and subsequent loss of kidney function in patients undergoing cardiac surgery: an observational cohort study.Lancet. 2019 Aug 10;394(10197):488-496. doi: 10.1016/S0140-6736(19)30769-X. Epub 2019 Jun 12. Lancet. 2019. PMID: 31202596
-
Effects of peri-operative nonsteroidal anti-inflammatory drugs on post-operative kidney function for adults with normal kidney function.Cochrane Database Syst Rev. 2018 Nov 29;11(11):CD011274. doi: 10.1002/14651858.CD011274.pub2. Cochrane Database Syst Rev. 2018. PMID: 30488949 Free PMC article.
-
Risk factors for acute kidney injury after pediatric cardiac surgery: a meta-analysis.Pediatr Nephrol. 2022 Mar;37(3):509-519. doi: 10.1007/s00467-021-05297-0. Epub 2021 Sep 30. Pediatr Nephrol. 2022. PMID: 34595570 Review.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
