

This is a preprint.
Investigating Ethical Tradeoffs in Crisis Standards of Care through Simulation of Ventilator Allocation Protocols
- PMID: 38559008
- PMCID: PMC10980139
- DOI: 10.1101/2024.03.10.24304058
Investigating Ethical Tradeoffs in Crisis Standards of Care through Simulation of Ventilator Allocation Protocols
Update in
-
Investigating ethical tradeoffs in crisis standards of care through simulation of ventilator allocation protocols.PLoS One. 2024 Sep 12;19(9):e0300951. doi: 10.1371/journal.pone.0300951. eCollection 2024. PLoS One. 2024. PMID: 39264928 Free PMC article.
Abstract
Introduction: Arguments over the appropriate Crisis Standards of Care (CSC) for public health emergencies often assume that there is a tradeoff between saving the most lives, saving the most life-years, and preventing racial disparities. However, these assumptions have rarely been explored empirically. To quantitatively characterize possible ethical tradeoffs, we aimed to simulate the implementation of five proposed CSC protocols for rationing ventilators in the context of the COVID-19 pandemic.
Methods: A Monte Carlo simulation was used to estimate the number of lives saved and life-years saved by implementing clinical acuity-, comorbidity- and age-based CSC protocols under different shortage conditions. This model was populated with patient data from 3707 adult admissions requiring ventilator support in a New York hospital system between April 2020 and May 2021. To estimate lives and life-years saved by each protocol, we determined survival to discharge and estimated remaining life expectancy for each admission.
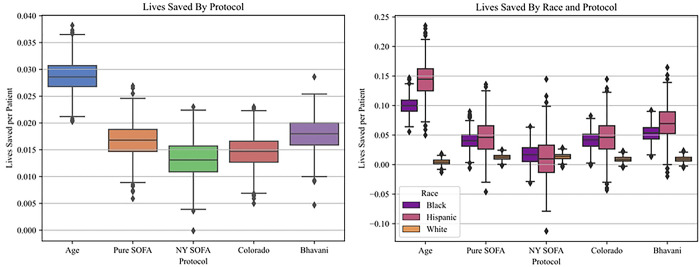
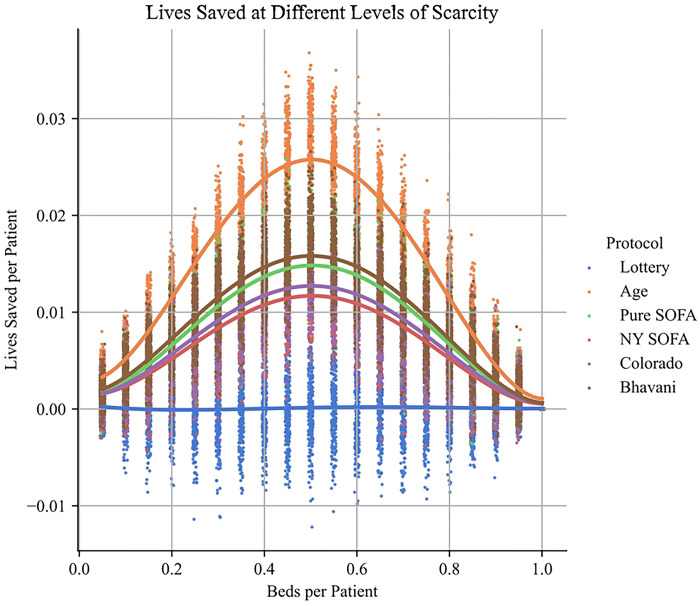
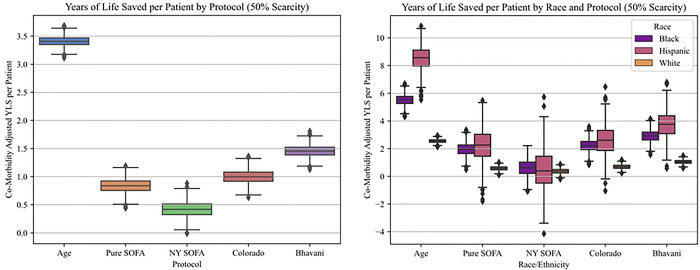
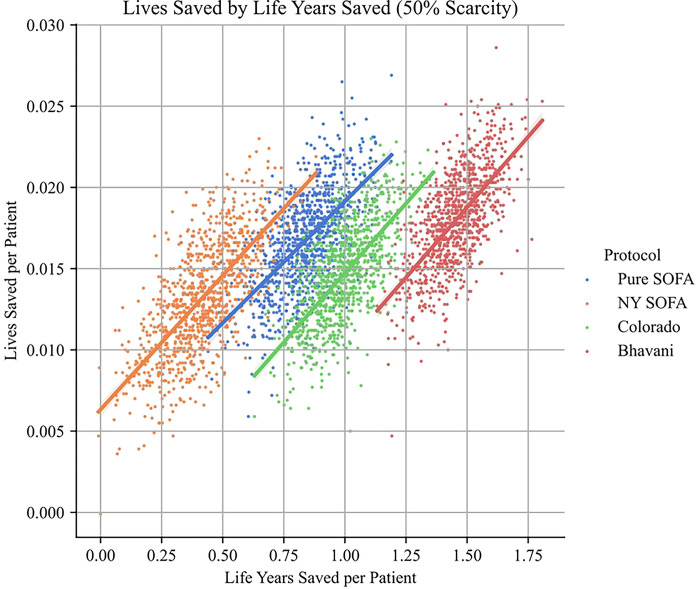
Results: The simulation demonstrated stronger performance for age- and comorbidity-sensitive protocols. For a capacity of 1 bed per 2 patients, ranking by age bands saves approximately 28.7 lives and 3408 life-years per thousand patients, while ranking by Sequential Organ Failure Assessment (SOFA) bands saved the fewest lives (13.2) and life-years (416). For all protocols, we observed a positive correlation between lives saved and life-years saved. For all protocols except lottery and the banded SOFA, significant disparities in lives saved and life-years saved were noted between White non-Hispanic, Black non-Hispanic, and Hispanic sub-populations.
Conclusion: While there is significant variance in the number of lives saved and life-years saved, we did not find a tradeoff between saving the most lives and saving the most life-years. Moreover, concerns about racial discrimination in triage protocols require thinking carefully about the tradeoff between enforcing equality of survival rates and maximizing the lives saved in each sub-population.
Figures
Similar articles
-
Investigating ethical tradeoffs in crisis standards of care through simulation of ventilator allocation protocols.PLoS One. 2024 Sep 12;19(9):e0300951. doi: 10.1371/journal.pone.0300951. eCollection 2024. PLoS One. 2024. PMID: 39264928 Free PMC article.
-
Accuracy of the Sequential Organ Failure Assessment Score for In-Hospital Mortality by Race and Relevance to Crisis Standards of Care.JAMA Netw Open. 2021 Jun 1;4(6):e2113891. doi: 10.1001/jamanetworkopen.2021.13891. JAMA Netw Open. 2021. PMID: 34143190 Free PMC article.
-
Quantifying Utilitarian Outcomes to Inform Triage Ethics: Simulated Performance of a Ventilator Triage Protocol under Sars-CoV-2 Pandemic Surge Conditions.AJOB Empir Bioeth. 2022 Jul-Sep;13(3):196-204. doi: 10.1080/23294515.2022.2063999. Epub 2022 Apr 18. AJOB Empir Bioeth. 2022. PMID: 35435803
-
Ethics of ICU triage during COVID-19.Br Med Bull. 2021 Jun 10;138(1):5-15. doi: 10.1093/bmb/ldab009. Br Med Bull. 2021. PMID: 34057458 Free PMC article. Review.
-
Improvement in trauma care for road traffic injuries: an assessment of the effect on mortality in low-income and middle-income countries.Lancet. 2022 Jul 23;400(10348):329-336. doi: 10.1016/S0140-6736(22)00887-X. Epub 2022 Jun 30. Lancet. 2022. PMID: 35779549 Review.
References
-
- New York State Task Force on Life and the Law. Ventilator Allocation Guidelines [Internet]. New York, N.Y.: NYS Department of Health; 2015. Nov [cited 2021 Jul 4]. Available from: https://www.health.ny.gov/regulations/task_force/reports_publications/do...
-
- Emanuel EJ, Persad G, Upshur R, Thome B, Parker M, Glickman A, et al. Fair Allocation of Scarce Medical Resources in the Time of Covid-19. New England Journal of Medicine. 2020. Mar 23;382(21):2049–55. - PubMed
-
- White DB, Lo B. A Framework for Rationing Ventilators and Critical Care Beds During the COVID-19 Pandemic. JAMA. 2020. May 12;323(18):1773. - PubMed
-
- Schmidt H, Roberts D, Eneanya N. Rationing, racism and justice: advancing the debate around “colourblind” COVID-19 ventilator allocation. Journal of medical ethics [Internet]. 2022. Feb [cited 2022 Mar 7];48(2). Available from: https://pubmed.ncbi.nlm.nih.gov/33408091/ - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous