

Case Report: Comprehensive evaluation of ECG phenotypes and genotypes in a family with Brugada syndrome carrying SCN5A-R376H
- PMID: 38559671
- PMCID: PMC10978698
- DOI: 10.3389/fcvm.2024.1334096
Case Report: Comprehensive evaluation of ECG phenotypes and genotypes in a family with Brugada syndrome carrying SCN5A-R376H
Abstract
Background: Brugada syndrome (BrS) is a channelopathy that can lead to sudden cardiac death in the absence of structural heart disease. Patients with BrS can be asymptomatic or present with symptoms secondary to polymorphic ventricular tachycardia or ventricular fibrillation. Even though BrS can exhibit autosomal dominant inheritance, it is not easy to identify the phenotype and genotype in a family thoroughly.
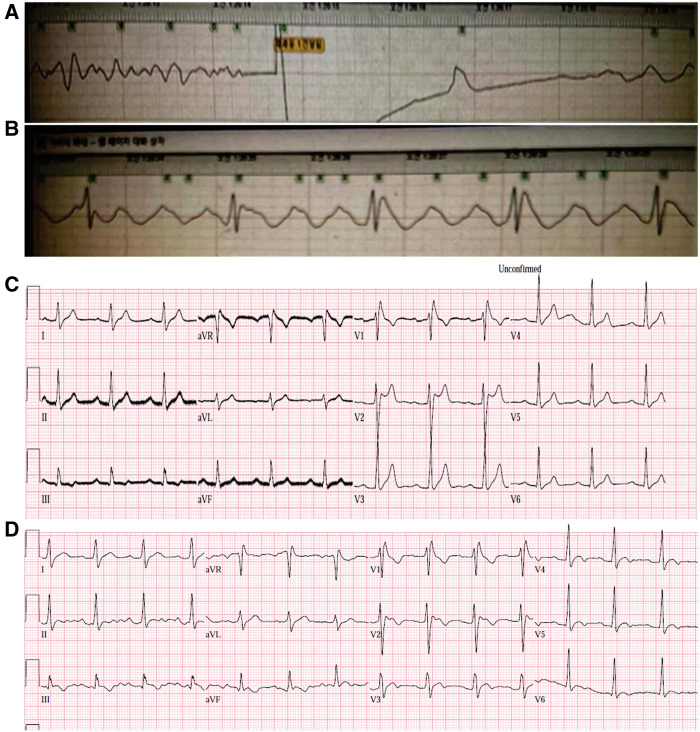
Case: We report the case of a 20-year-old man with variants in SCN5A and RyR2 genes who was resuscitated from sudden cardiac death during sleep due to a ventricular fibrillation. The patient did not have underlying diseases. The routine laboratory results, imaging study, coronary angiogram, and echocardiogram (ECG) were normal. A type 1 BrS pattern was identified in one resting ECG. Furthermore, prominent J wave accentuation with PR interval prolongation was identified during therapeutic hypothermia. Therefore, we were easily able to diagnose BrS. For secondary prevention, the patient underwent implantable cardioverter defibrillator implantation. Before discharge, a genetic study was performed using next-generation sequencing. Genotyping was performed in the first-degree relatives, and ECG evaluations of almost all maternal and paternal family members were conducted. The proband and his mother showed SCN5A-R376H and RyR2-D4038Y variants. However, his mother did not show the BrS phenotype on an ECG. One maternal aunt and uncle showed BrS phenotypes.
Conclusion: Genetics alone cannotdiagnose BrS. However, genetics could supply evidence or direction for evaluating ECG phenotypes in family groups. This case report shows how family evaluation using ECGs along with a genetic study can be used in BrS diagnosis.
Keywords: Brugada syndrome; SCN5A; family screening; genetic study; sudden cardiac death.
© 2024 Ly, Kim, Lee, Yoon and Park.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous