

Severe Elevated Bile Acids in Early Pregnancy
- PMID: 38560018
- PMCID: PMC10977523
- DOI: 10.14309/crj.0000000000001317
Severe Elevated Bile Acids in Early Pregnancy
Abstract
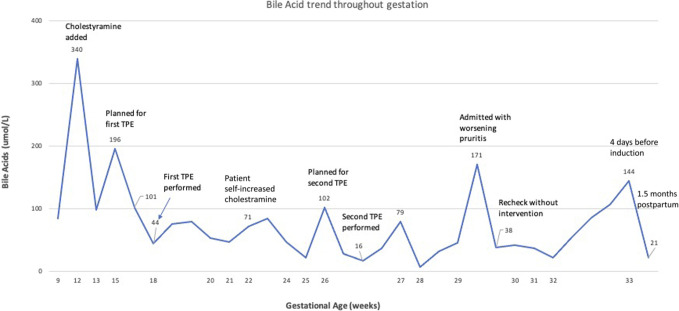
Intrahepatic cholestasis of pregnancy (ICP) typically presents in the second half of pregnancy. Severe ICP is associated with increased risk of stillbirth. Little is known regarding elevated bile acids in the first trimester. We present a case of severely elevated bile acids in the first trimester, resistant to conservative management, in a patient with pre-existing cholestatic liver disease and aortic valve disease requiring anticoagulation. Therapeutic plasma exchange was used. In those with pre-existing cholestatic disease, early bile acid elevation is likely distinct from ICP, and conservative strategies may not be useful. In addition, therapeutic enoxaparin appears safe in therapeutic plasma exchange.
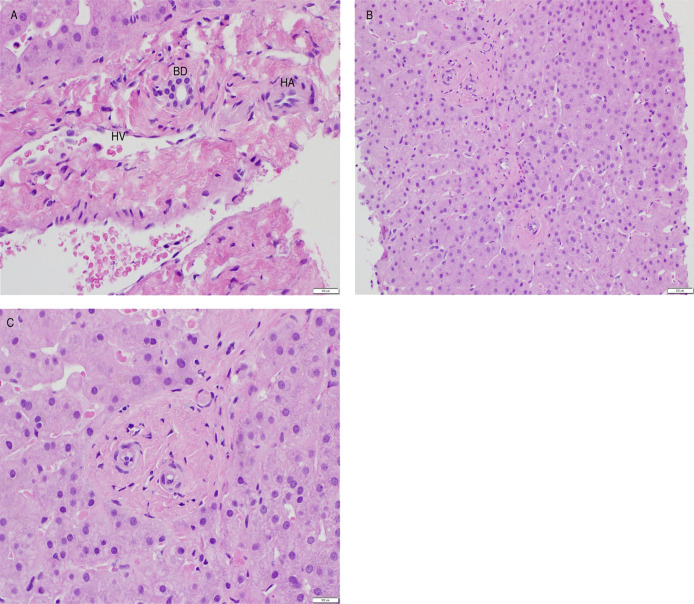
Keywords: Bile acids; Pregnancy; ductopenia; ntrahepatic cholestasis of pregnancy; vanishing bile duct syndrome.
© 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The American College of Gastroenterology.
Figures
Similar articles
-
Intrahepatic Cholestasis of Pregnancy: A Case Report of Third-Trimester Onset of the Disease.Cureus. 2022 Nov 27;14(11):e31926. doi: 10.7759/cureus.31926. eCollection 2022 Nov. Cureus. 2022. PMID: 36580079 Free PMC article.
-
[Clinical practice guidelines of the Team of Experts of the Polish Gynecological Society: management of the intrahepatic cholestasis of pregnancy].Ginekol Pol. 2012 Sep;83(9):713-7. Ginekol Pol. 2012. PMID: 23342903 Polish.
-
Infliximab-Induced Vanishing Bile Duct Syndrome.Cureus. 2022 Feb 5;14(2):e21940. doi: 10.7759/cureus.21940. eCollection 2022 Feb. Cureus. 2022. PMID: 35273881 Free PMC article.
-
Bile acids and progesterone metabolites in intrahepatic cholestasis of pregnancy.Ann Med. 2000 Mar;32(2):94-106. doi: 10.3109/07853890009011758. Ann Med. 2000. PMID: 10766400 Review.
-
Genetic cholestasis: lessons from the molecular physiology of bile formation.Can J Gastroenterol. 2000 Mar;14(3):233-8. doi: 10.1155/2000/514172. Can J Gastroenterol. 2000. PMID: 10758420 Review.
Cited by
-
Intrahepatic cholestasis of pregnancy.Nat Rev Dis Primers. 2025 Jul 24;11(1):51. doi: 10.1038/s41572-025-00633-2. Nat Rev Dis Primers. 2025. PMID: 40707479 Review.
References
-
- Ovadia C, Seed PT, Sklavounos A, et al. Association of adverse perinatal outcomes of intrahepatic cholestasis of pregnancy with biochemical markers: Results of aggregate and individual patient data meta-analyses. Lancet. 2019;393(10174):899–909. Erratum in: Lancet. 2019;393(10176):1100. - PMC - PubMed
-
- Vasavan T, Williamson C, Chapter 65–sex and cardiac electrophysiology: Fetal arrhythmia in intrahepatic cholestasis of pregnancy In: Malik M. (eds). Sex and Cardiac Electrophysiology, Academic Press, Elsevier USA, Philidelphia PA, USA: 2020, 727–35, ISBN 9780128177280.
-
- Kaplan AA. Therapeutic plasma exchange: Core curriculum 2008. Am J Kidney Dis. 2008;52(6):1180–96. - PubMed
-
- Mathias A, Wax JR, Pinette MG, Cartin A, Blackstone J. Progressive familial intrahepatic cholestasis complicating pregnancy. J Matern Fetal Neonatal Med. 2009;22(9):816–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
