

Intracardiac masses: Single center experience within 12 years: I-MASS Study
- PMID: 38560087
- PMCID: PMC10978191
- DOI: 10.1016/j.ahjo.2021.100081
Intracardiac masses: Single center experience within 12 years: I-MASS Study
Abstract
Objective: The aim of this cross-sectional, retrospective, descriptive study was to review and classify cardiac masses systematically and to determine their frequencies.
Methods: The medical records of 64,862 consecutive patients were investigated within 12 years. Every patient with a cardiac mass imaged by transthoracic echocardiography (TTE) and confirmed with an advanced imaging modality such as transesophageal echocardiography (TEE), computed tomography (CT) and/or cardiac magnetic resonance imaging (CMR) was included. Acute coronary syndromes triggering thrombus formation, vegetations, intracardiac device and catheter related thrombi were excluded.
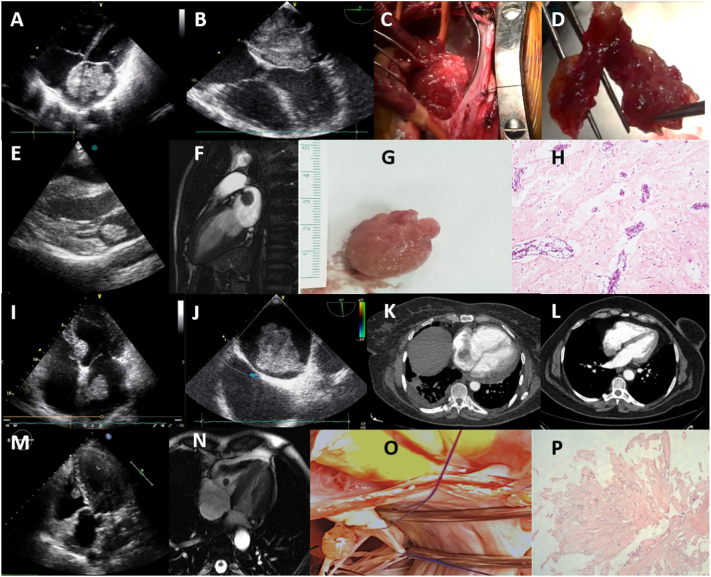
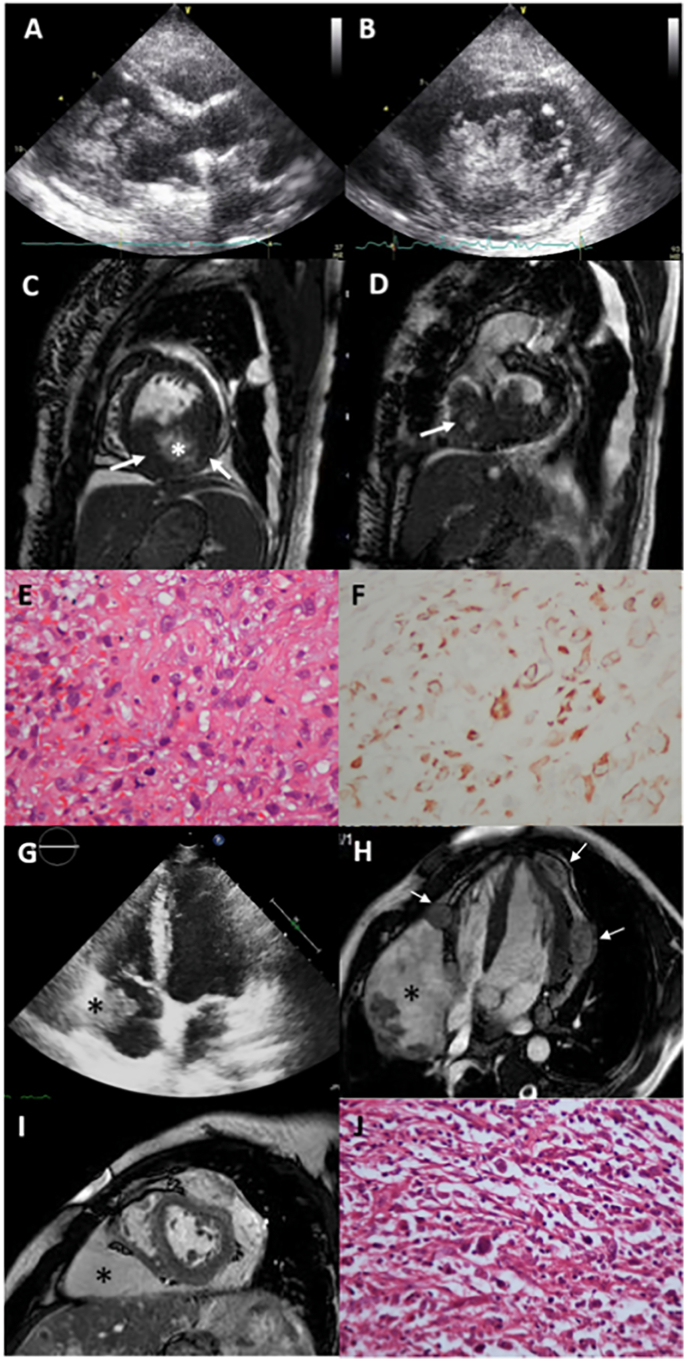
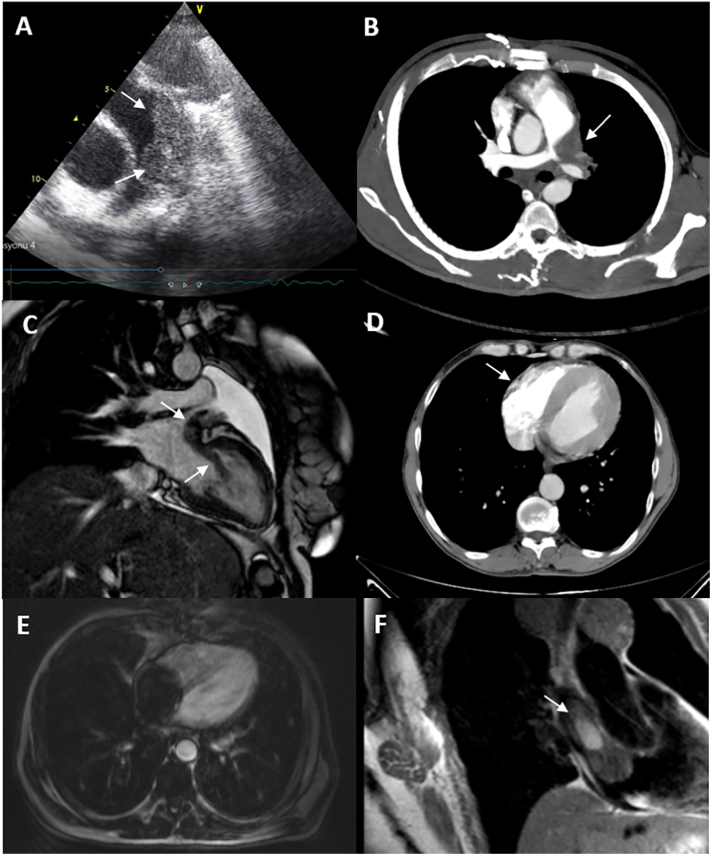
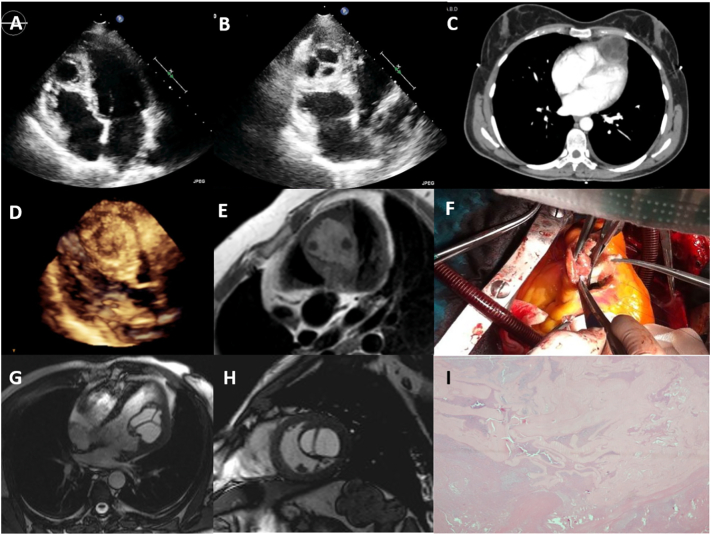
Results: Data demonstrated 127 (0.195%) intracardiac masses consisting of 33 (0.050%) primary benign, 3 (0.004%) primary malignant, 20 (0.030%) secondary tumors, 3 (0.004%) hydatid cysts and 68 (0.104%) thrombi respectively. The majority of primary cardiac tumors were benign (91.67%), predominantly myxomas (78.79%), and the less malignant (8.33%). Secondary cardiac tumors were common than the primary malignant tumors (20:3), with male dominancy (55%), lymphoma and lung cancers were the most frequent. Intracardiac thrombi was the majority of the cardiac masses, thrombi accompanying malignancies were in the first range (n = 17, 25%), followed by autoimmune diseases (n = 13, 19.12%) and ischemic heart disease with low ejection fraction (n = 12, 17.65%).
Conclusions: This retrospective analysis identified 127 patients with cardiac masses. The majority of benign tumors were myxoma, the most common tumors that metastasized to the heart were lymphoma and lung cancers, and the thrombi associated with malignancies and autoimmune diseases were the most frequent.
Keywords: Cardiac cysts; Cardiac thrombus; I-MASS Study; Primary cardiac tumors; Secondary cardiac tumors.
© 2021 Published by Elsevier Inc.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Reynen K. Frequency of primary tumors of the heart. Am. J. Cardiol. 1996;77:107. - PubMed
-
- Gowda R.M., Khan I.A., Nair C.K., Mehta N.J., Vasavada B.C., Sacchi T.J. Cardiac papillary fibroelastoma: a comprehensive analysis of 725 cases. Am. Heart J. 2003;146:404–410. - PubMed
-
- Strecker T., Rösch J., Weyand M., Agaimy A. Primary and metastatic cardiac tumors: imaging characteristics, surgical treatment, a histopathological spectrum: a 10 year-experience at a german heart center. Cardiovasc. Pathol. 2012;21:436–443. - PubMed
-
- Hudzik B., Miszalski-Jamka K., Glowacki J., Glowacki J., Lekston A., Gierlotka M., Zembala M., Polonski L., Gasior M. Malignant tumors of the heart. Cancer Epidemiol. 2015;39:665–672. - PubMed
-
- Yu L., Gu T., Shi E. Echocardiographic findings and clinical correlation with cardiac myxoma. J. Am. Coll. Cardiol. Imaging. 2016;9:618–620. - PubMed
LinkOut - more resources
Full Text Sources
