

Treatment switches of disease-modifying therapies in people with multiple sclerosis: long-term experience from the German MS Registry
- PMID: 38560408
- PMCID: PMC10981260
- DOI: 10.1177/17562864241239740
Treatment switches of disease-modifying therapies in people with multiple sclerosis: long-term experience from the German MS Registry
Abstract
Background: The spectrum of disease-modifying therapies (DMTs) for people with multiple sclerosis (PwMS) has expanded over years, but data on treatment strategies is largely lacking. DMT switches are common clinical practice.
Objective: To compare switchers and non-switchers, characterize the first DMT switch and identify reasons and predictors for switching the first DMT.
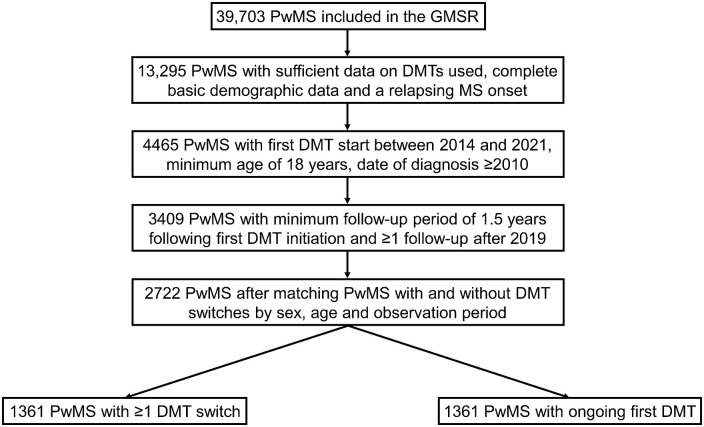
Methods: Data on 2722 PwMS from the German MS Registry were retrospectively analyzed regarding sociodemographic/clinical differences between 1361 switchers (PwMS discontinuing the first DMT) and non-switchers matched according to age, sex, and observation period. Frequencies of first and second DMTs were calculated and switch reasons identified. Predictors for DMT switches were revealed using univariable and multivariable regression models.
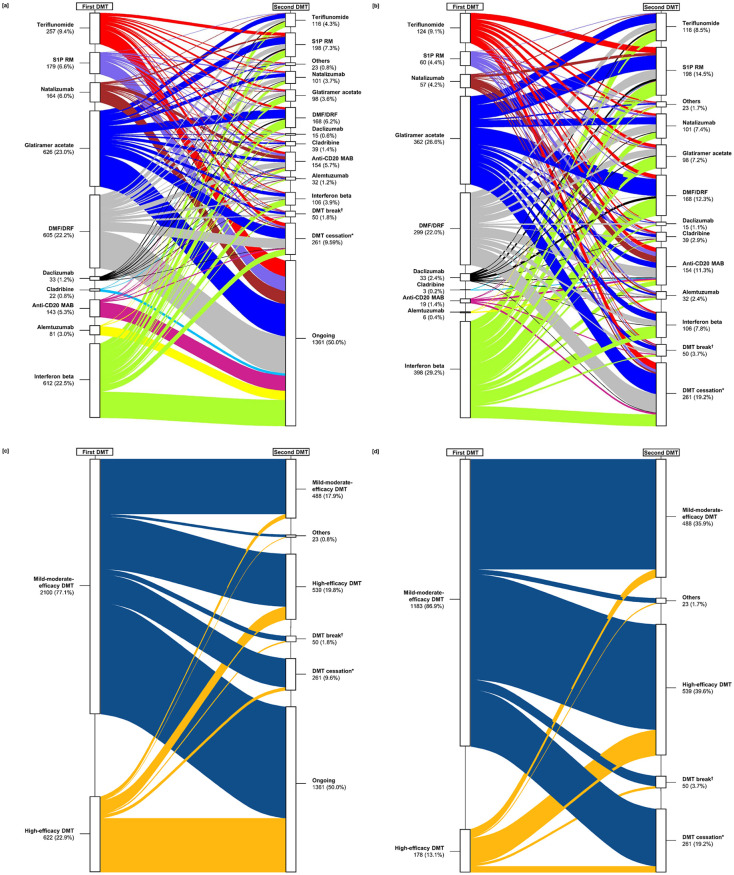
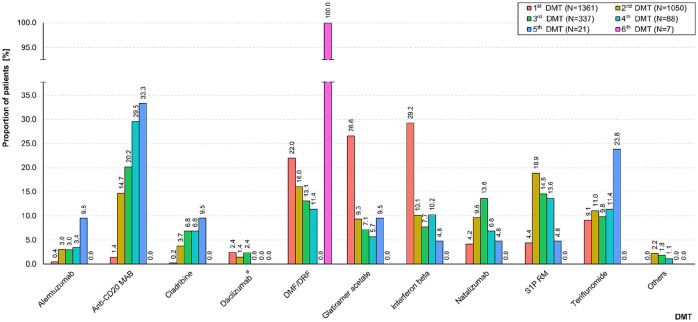
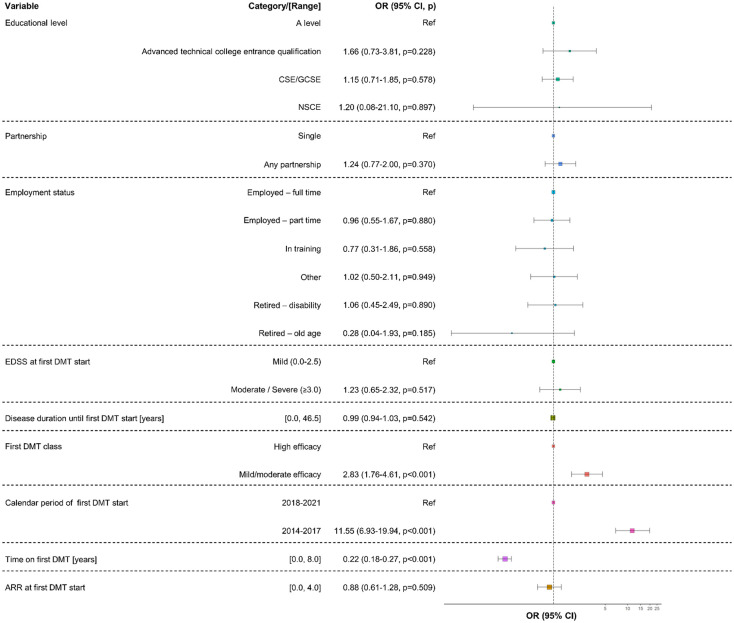
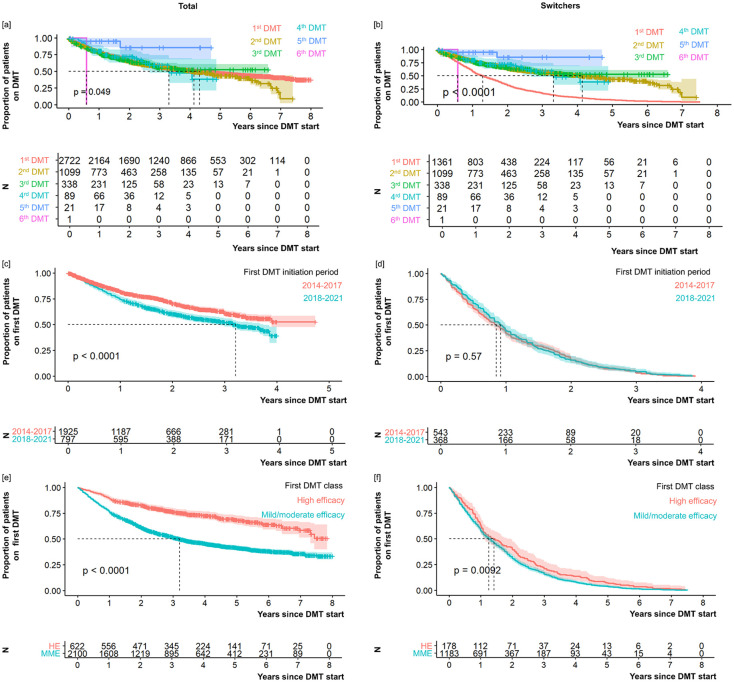
Results: Switchers and non-switchers differed significantly regarding time to first DMT, education, calendar period of the first DMT start (2014-2017 versus 2018-2021), first DMT class used [mild-to-moderate efficacy (MME) versus high-efficacy (HE) DMT], time on first DMT, and disease activity at first DMT start or cessation/last follow-up. The majority of PwMS started with MME DMTs (77.1%), with the most common being glatiramer acetate, dimethyl/diroximel fumarate, and beta-interferon variants. Switchers changed treatment more often to HE DMTs (39.6%), most commonly sphingosine-1-phosphate receptor modulators, anti-CD20 monoclonal antibodies, and natalizumab. Fewer PwMS switched to MME DMTs (35.9%), with the most common being dimethyl/diroximel fumarate, teriflunomide, or beta-interferon. Among 1045 PwMS with sufficient data (76.8% of 1361 switchers), the most frequent reasons for discontinuing the first DMT were disease activity despite DMT (63.1%), adverse events (17.1%), and patient request (8.3%). Predictors for the first DMT switch were MME DMT as initial treatment [odds ratio (OR) = 2.83 (1.76-4.61), p < 0.001; reference: HE DMT], first DMT initiation between 2014 and 2017 [OR = 11.55 (6.93-19.94), p < 0.001; reference: 2018-2021], and shorter time on first DMT [OR = 0.22 (0.18-0.27), p < 0.001].
Conclusion: The initial use of MME DMTs was among the strongest predictors of DMT discontinuation in a large German retrospective MS cohort, arguing for the need for prospective treatment strategy trials, not only but also on the initial broad use of HE DMTs in PwMS.
Keywords: discontinuation; disease-modifying therapy; multiple sclerosis; switch.
© The Author(s), 2024.
Figures
References
-
- Filippi M, Bar-Or A, Piehl F, et al.. Multiple sclerosis. Nat Rev Dis Primers 2018; 4: 43. - PubMed
-
- MS International Federation (MSIF). Number of people with MS | Atlas of MS, https://www.atlasofms.org/map/global/epidemiology/number-of-people-with-ms (accessed 15 January 2024).
-
- Gilmour H, Ramage-Morin PL, Wong SL. Multiple sclerosis: prevalence and impact. Health Rep 2018; 29: 3–8. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
