

The contribution of estimated dead space fraction to mortality prediction in patients with chronic obstructive pulmonary disease-a new proposal
- PMID: 38560478
- PMCID: PMC10981412
- DOI: 10.7717/peerj.17081
The contribution of estimated dead space fraction to mortality prediction in patients with chronic obstructive pulmonary disease-a new proposal
Abstract
Background: Mortality due to chronic obstructive pulmonary disease (COPD) is increasing. However, dead space fractions at rest (VD/VTrest) and peak exercise (VD/VTpeak) and variables affecting survival have not been evaluated. This study aimed to investigate these issues.
Methods: This retrospective observational cohort study was conducted from 2010-2020. Patients with COPD who smoked, met the Global Initiatives for Chronic Lung Diseases (GOLD) criteria, had available demographic, complete lung function test (CLFT), medication, acute exacerbation of COPD (AECOPD), Charlson Comorbidity Index, and survival data were enrolled. VD/VTrest and VD/VTpeak were estimated (estVD/VTrest and estVD/VTpeak). Univariate and multivariable Cox regression with stepwise variable selection were performed to estimate hazard ratios of all-cause mortality.
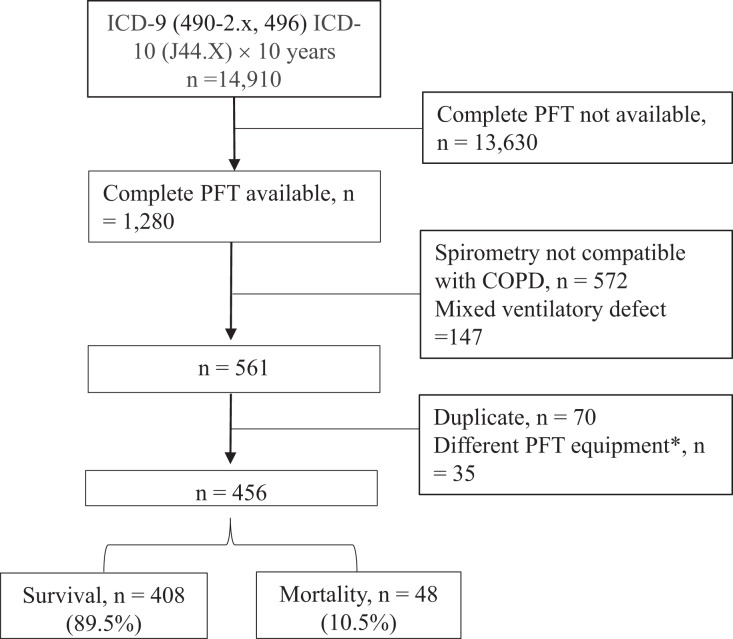
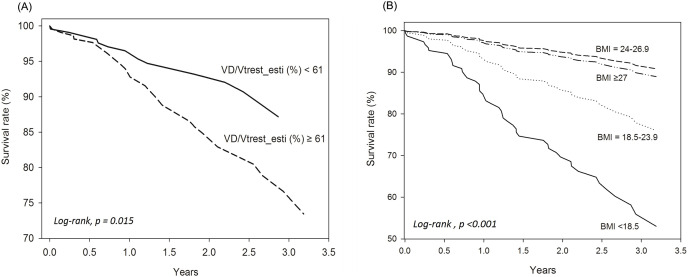
Results: Overall, 14,910 patients with COPD were obtained from the hospital database, and 456 were analyzed after excluding those without CLFT or meeting the lung function criteria during the follow-up period (median (IQR) 597 (331-934.5) days). Of the 456 subjects, 81% had GOLD stages 2 and 3, highly elevated dead space fractions, mild air-trapping and diffusion impairment. The hospitalized AECOPD rate was 0.60 ± 2.84/person/year. Forty-eight subjects (10.5%) died, including 30 with advanced cancer. The incidence density of death was 6.03 per 100 person-years. The crude risk factors for mortality were elevated estVD/VTrest, estVD/VTpeak, ≥2 hospitalizations for AECOPD, advanced age, body mass index (BMI) <18.5 kg/m2, and cancer (hazard ratios (95% C.I.) from 1.03 [1.00-1.06] to 5.45 [3.04-9.79]). The protective factors were high peak expiratory flow%, adjusted diffusing capacity%, alveolar volume%, and BMI 24-26.9 kg/m2. In stepwise Cox regression analysis, after adjusting for all selected factors except cancer, estVD/VTrest and BMI <18.5 kg/m2 were risk factors, whereas BMI 24-26.9 kg/m2 was protective. Cancer was the main cause of all-cause mortality in this study; however, estVD/VTrest and BMI were independent prognostic factors for COPD after excluding cancer.
Conclusions: The predictive formula for dead space fraction enables the estimation of VD/VTrest, and the mortality probability formula facilitates the estimation of COPD mortality. However, the clinical implications should be approached with caution until these formulas have been validated.
Keywords: Acute exacerbation; Co-morbidity; Dead space and tidal volume ratio; Lung function; Mortality.
© 2024 Chuang et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Prediction and types of dead-space fraction during exercise in male chronic obstructive pulmonary disease patients.Medicine (Baltimore). 2022 Feb 11;101(6):e28800. doi: 10.1097/MD.0000000000028800. Medicine (Baltimore). 2022. PMID: 35147114 Free PMC article.
-
[Evaluation of the respiratory system in patients with heart failure based on spiro-ergometric exercise test parameters].Przegl Lek. 2002;59(8):568-71. Przegl Lek. 2002. PMID: 12638321 Clinical Trial. Polish.
-
Hierarchical stratification of the factors related to exertional dyspnoea and exercise intolerance in male COPD patients.Ann Med. 2022 Dec;54(1):2941-2950. doi: 10.1080/07853890.2022.2135018. Ann Med. 2022. PMID: 36314466 Free PMC article.
-
Tidal volume expandability and ventilatory efficiency as predictors of mortality in Taiwanese male patients with chronic obstructive pulmonary disease: A 10-year follow-up study - Is V̇O2peak or FEV1% the gold standard?Chron Respir Dis. 2023 Jan-Dec;20:14799731231220675. doi: 10.1177/14799731231220675. Chron Respir Dis. 2023. PMID: 38086393 Free PMC article.
-
Once daily long-acting beta2-agonists and long-acting muscarinic antagonists in a combined inhaler versus placebo for chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2019 Mar 6;3(3):CD012930. doi: 10.1002/14651858.CD012930.pub2. Cochrane Database Syst Rev. 2019. PMID: 30839102 Free PMC article.
References
-
- Burrows B, Kasik JE, Niden AH, Barclay WR. Clinical usefulness of the single breath pulmonary diffusing capacity test. American Review of Respiratory Disease. 1961;84:789–806. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
