

Ten year real world experience with ultrafiltration for the management of acute decompensated heart failure
- PMID: 38560637
- PMCID: PMC10978396
- DOI: 10.1016/j.ahjo.2022.100230
Ten year real world experience with ultrafiltration for the management of acute decompensated heart failure
Abstract
Background: Randomized controlled trials (RCT) of ultrafiltration (UF) have demonstrated conflicting results regarding its efficacy and safety.
Objective: We reviewed 10 years of data for adjustable UF during heart failure hospitalizations in a real world cohort.
Methods: We performed a retrospective, single center analysis of 335 consecutive patients treated with adjustable rate UF using the CHF Solutions Aquadex Flex Flo System from 2009 to 2019.
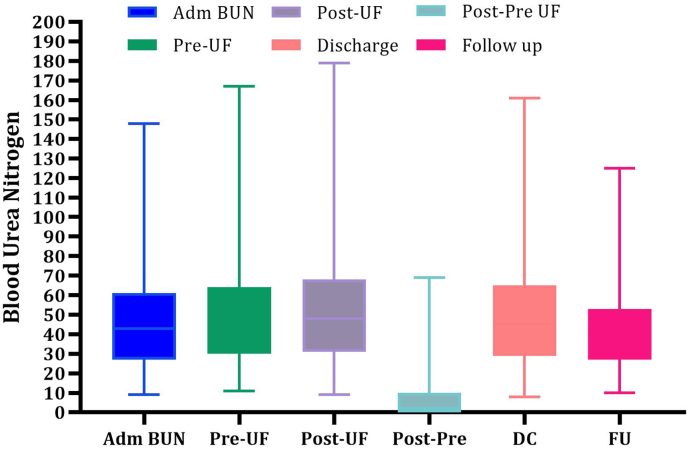
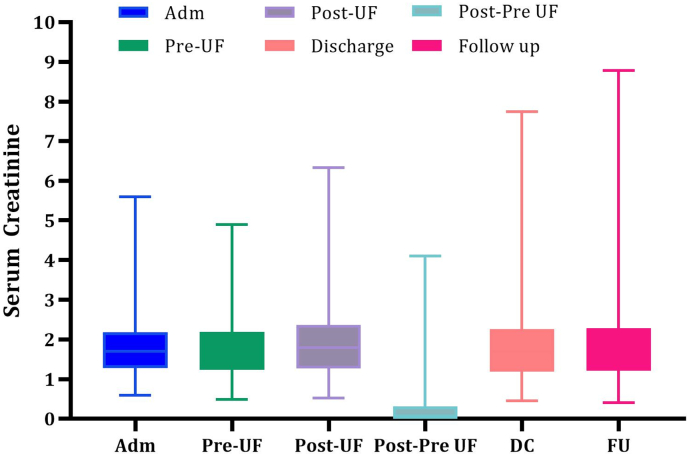
Results: Compared to previous RCTs investigating UF, our cohort was older, with worse renal impairment and more antecedent HF hospitalizations in the year preceding therapy. Mean fluid removal with UF was 14.6 l. Mean weight loss with UF was 15.6 lbs (range 0.2-57 lbs) and was sustained at 1-2 week follow-up. Mean creatinine change upon stopping UF, at discharge and follow-up (mean 30 days) was +0.11 mg/dl, +0.07 mg/dl and +0.11 mg/dl, respectively. HF rehospitalizations at 30 days, 90 days and 1 year were 12.4 %, 14.9 % and 27.3 % respectively. On average patients had 1.74 fewer hospitalizations for HF in the year following UF when compared to 12 months preceding UF. Major bleeding defined as requiring discontinuation of anticoagulation occurred in 3.6 % of patients.
Conclusions: Compared with previous UF trials, our study demonstrates that UF compares favorably for HF rehospitalizations, renal function response, and weight/volume loss. Importantly, our real world experience allowed for the adjustment of UF rate during therapy and we believe this is a major contributor to our favorable outcomes. In clinical practice, UF can be a safe and effective strategy for decongestion.
Keywords: Aquapheresis; Decongestion; Heart failure; Ultrafiltration.
© 2022 Published by Elsevier Inc.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Maureen Hummel reports financial support was provided by CHF Solutions (Nuwellis) for independent data analysis. Maureen Hummel reports a relationship with CHF Solutions (Nuwellis) that includes: speaking and lecture fees and travel reimbursement.
Figures
References
-
- Virani S.S., Alonso A., Benjamin E.J., Bittencourt M.S., Callaway C.W., Carson A.P., Chamberlain A.M., Chang A.R., Cheng S., Delling F.N., Djousse L., Elkind M.S.V., Ferguson J.F., Fornage M., Khan S.S., Kissela B.M., Knutson K.L., Kwan T.W., Lackland D.T., Lewis T.T., Lichtman J.H., Longenecker C.T., Loop M.S., Lutsey P.L., Martin S.S., Matsushita K., Moran A.E., Mussolino M.E., Perak A.M., Rosamond W.D., Roth G.A., Sampson U.K.A., Satou G.M., Scroeder E.B., Shah S.H., Shay C.M., Spartano N.L., Stokes A., Tirschwell D.L., VanWagner L.B., Tsao C.W. Heart disease and stroke statistics: 2020 update-a report for the American Heart Association. Circ. 2020 Mar 3;141(9) e139- e596. - PubMed
-
- Lala A., McNulty S.E., Mentz R.J., Dunlay S.M., Vader J.M., AbouEzzedine OF. DeVore A.D., Khazanie P., Redfield M.M., Goldsmith S.R., Bradley B.A., Anstrom K.J., Felker G.M., Hernandez A.F., Stevenson L.W. Relief and recurrence of congestion during and after hospitalization for acute heart failure. Insights from Diuretic Optimization Strategy Evaluation in Acute Decompensate Heart Failure (DOSE-AHF) and Cardiorenal Rescue Study in Acute Decompensated Heart Failure (CARRESS-HF) Circ. Heart Fail. 2015;8:741–748. - PMC - PubMed
-
- Schrier R.W. Role of diminished renal function in cardiovascular mortality: marker or pathogenetic factor? J. Am. Coll. Cardiol. 2006;47(1):1–8. - PubMed
-
- Costanzo M.R., Guglin M.E., Saltzberg M.T., Jessup M.L., Bart B.A., Teerlink J.R., Jaski B.E., Fang J.C., Feller E.D., Haas G.J., Anderson A.S., Schollmeyer M.P., Sobotka P.A. Ultrafiltration versus intravenous diuretics patients hospitalized for acute decompensated heart failure. J. Am. Coll. Cardiol. 2007;49(6):675–683. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
