

Clinical spectrum and evolution of immune-checkpoint inhibitors toxicities over a decade-a worldwide perspective
- PMID: 38560659
- PMCID: PMC10981010
- DOI: 10.1016/j.eclinm.2024.102536
Clinical spectrum and evolution of immune-checkpoint inhibitors toxicities over a decade-a worldwide perspective
Abstract
Background: Immune-checkpoint inhibitors (ICI) have revolutionized cancer treatment by harnessing the immune system but ICI can induce life-threatening immune-related adverse events (irAE) affecting every organ.
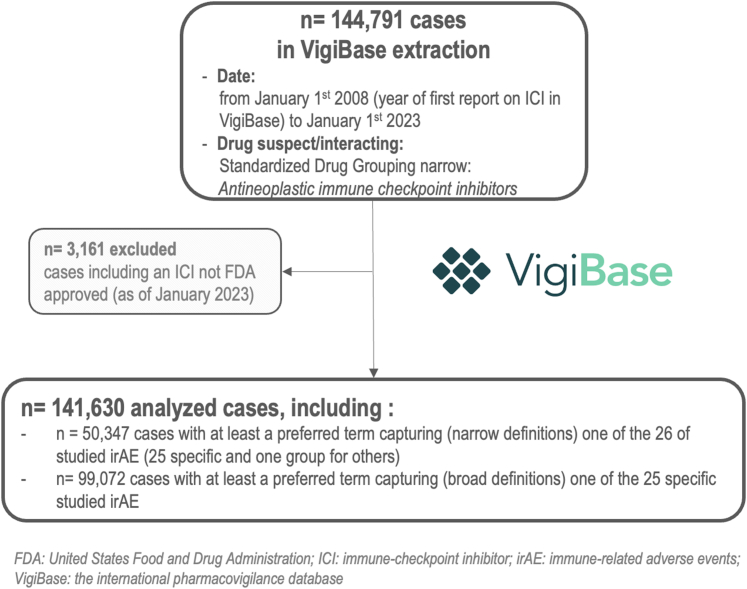
Methods: We extracted irAE from VigiBase, the international pharmacovigilance database, first reported in 2008 until 01/2023 to characterize irAE reporting trends, clinical features, risk factors and outcomes.
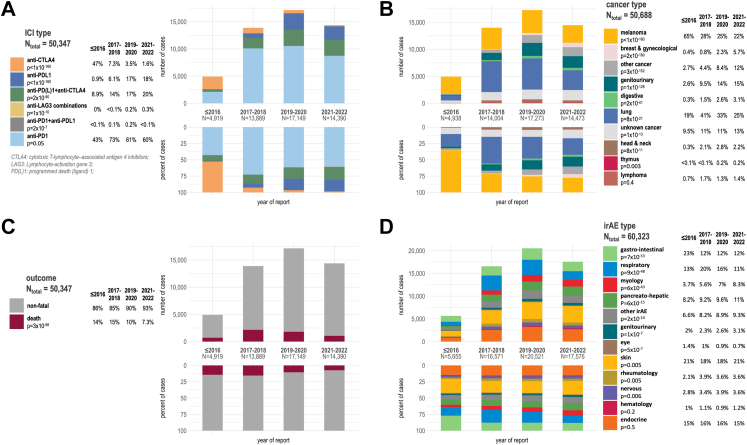
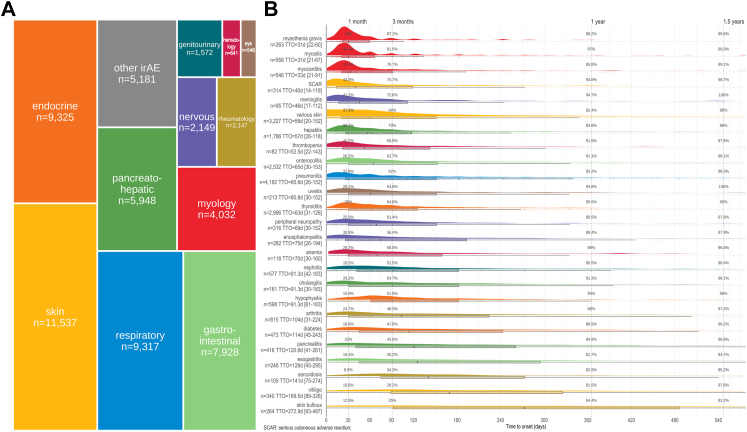
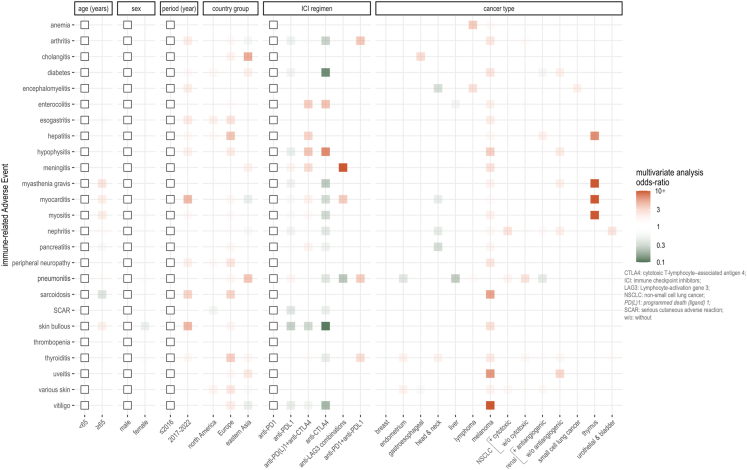
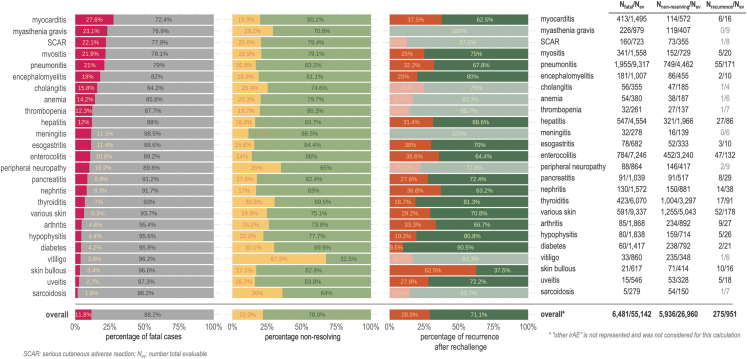
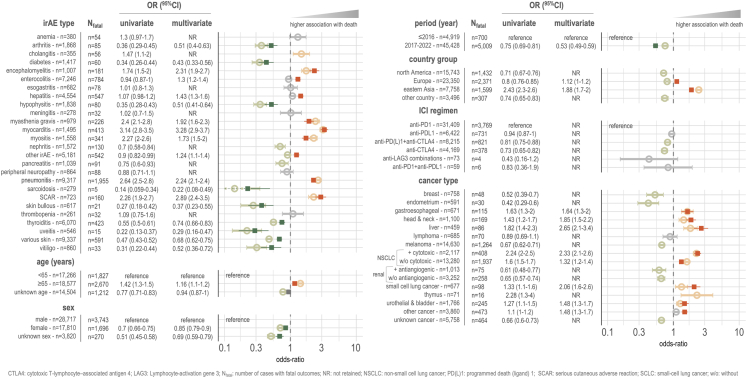
Findings: We distinguished 25 types of irAE (n = 50,347cases, single irAE/case in 84.9%). Cases mainly involved anti-PD1 (programmed-death-1) monotherapy (62.4%) in male (61.7%) aged 64.3 ± 12.6 years. After 2020 vs. prior to 2016, proportion of anti-CTLA4 (Cytotoxic-T-Lymphocyte-Antigen-4) monotherapy prescription almost vanished (1.6% vs. 47%, respectively) contrasting with increased use of anti-PDL1 (PD1-ligand) monotherapy (18% vs. 0.9%) and anti-CTLA4+anti-PD(L)1 combination (20% vs. 8.9%). Anti-LAG3 (Lymphocyte-Activation-Gene-3) prescription was limited (<1%) in the studied timeframe. After 2020, over 14 different cancer types were treated vs. almost exclusively melanoma and lung cancers before 2016. Overall, the most reported irAE were skin reactions (22.9%), pneumonitis (18.5%), enterocolitis (14.4%) and thyroiditis (12.1%). ICI-myotoxicities (6.6%) included myositis, myocarditis and myasthenia-gravis like syndrome and were the most overlapping irAE (up to 30% overlap, vs. <3% in general for other inter-irAE overlap). The top factors associated with specific irAE (odds-ratio>5) were presence of thymic cancer for ICI-myotoxicities or hepatitis; presence of melanoma for vitiligo, uveitis or sarcoidosis; specific types of ICI regimen (anti-LAG3 for meningitis, anti-CTLA4 for hypophysitis); and specific reporting regions (eastern Asia for cholangitis). Median time-to-onset ranged from 31 to 273 days, being shortest for myotoxicities and most delayed for skin-bullous auto-immune reactions. Overall fatality was highest for myocarditis = 27.6%, myasthenia = 23.1%, severe cutaneous adverse reactions (SCAR) = 22.1%, myositis = 21.9%, pneumonitis = 21%, and encephalomyelitis = 18%; generally decreasing after 2020, except for myasthenia and SCAR. When reported, irAE recurrence rate after rechallenge was 28.9% (n = 275/951).
Interpretation: This up-to-date comprehensive worldwide pharmacovigilance study defines the spectrum, characteristics, and evolution of irAE reporting summarizing over a decade of use. Multiple risk factors and clinical peculiarities for specific irAE have been identified as signals to guide clinical practice and future research.
Funding: Paul Gougis was supported by the academic program: "Contrats ED: Programme blanc Institut Curie PSL" for the conduct of his PhD. Baptiste Abbar was supported by "the Fondation ARC Pour le Rechercher Sur le Cancer". The RT2L research group (Institut Curie) was supported by the academic program "SHS INCa", Sanofi iTech award, and by Monoprix∗.
Keywords: Cancer; Fatal; Immune checkpoint inhibitors; Immune-related adverse events; Myotoxicity; Pharmacology; Pharmacovigilance.
© 2024 The Author(s).
Conflict of interest statement
Dr Gougis declares participation to advisory board from BMS, travel support from Eisai, and an academic grant from Sanofi. Dr Abbar reports consulting fees or honoraria from Novartis, AstraZeneca, BMS, MSD, Astellas, and Sanofi. Dr Salem have participated to advisory boards, consultancy or received grants from BMS, Novartis, AstraZeneca, CRC-Oncology, EISAI, IPSEN, Bayer, Banook Group, and BeiGene. Dr Spano have participated to advisory boards, consultancy from Roche, MSD, BMS, Lilly, AstraZeneca, Daiichi-Sankyo, Mylan, Novartis, Pfizer, PFO, LeoPharma and Gilead, and Grant for MSDAvenir. Dr Moslehi served on advisory boards for Bristol-Myers Squibb, Takeda, AstraZeneca, Myovant, Kurome Therapeutics, Kiniksa Pharmaceuticals, Daiichi Sankyo, CRC Oncology, BeiGene, Prelude Therapeutics, TransThera Sciences, BitterRoot Bio, Deciphera, Regeneron, Teva and Cytokinetics and is supported by the NIH (R01HL141466, R01HL155990, R01HL156021, R01 HL160688, R01 HL170038). All other authors report no COI.
Figures
References
-
- Geraud A., Gougis P., Vozy A., et al. Clinical pharmacology and interplay of immune checkpoint agents: a yin-yang balance. Annu Rev Pharmacol Toxicol. 2021;61:85–112. - PubMed
-
- Postow M.A., Sidlow R., Hellmann M.D. Immune-related adverse events associated with immune checkpoint blockade. N Engl J Med. 2018;378:158–168. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
