

Isolated unilateral alar ligamentous injury: illustrative cases
- PMID: 38560931
- PMCID: PMC10988229
- DOI: 10.3171/CASE23664
Isolated unilateral alar ligamentous injury: illustrative cases
Abstract
Background: Isolated unilateral alar ligament injury (IUALI) is a rare and likely underreported occurrence after upper cervical trauma, with only 16 cases documented in the literature to date. Patients generally present with neck pain, and definitive diagnosis is typically made by magnetic resonance imaging (MRI). Unfortunately, likely due in part to its rarity, there are no formal guidelines for the treatment of an IUALI. Furthermore, there is a limited understanding of the long-term consequences associated with its inadequate treatment.
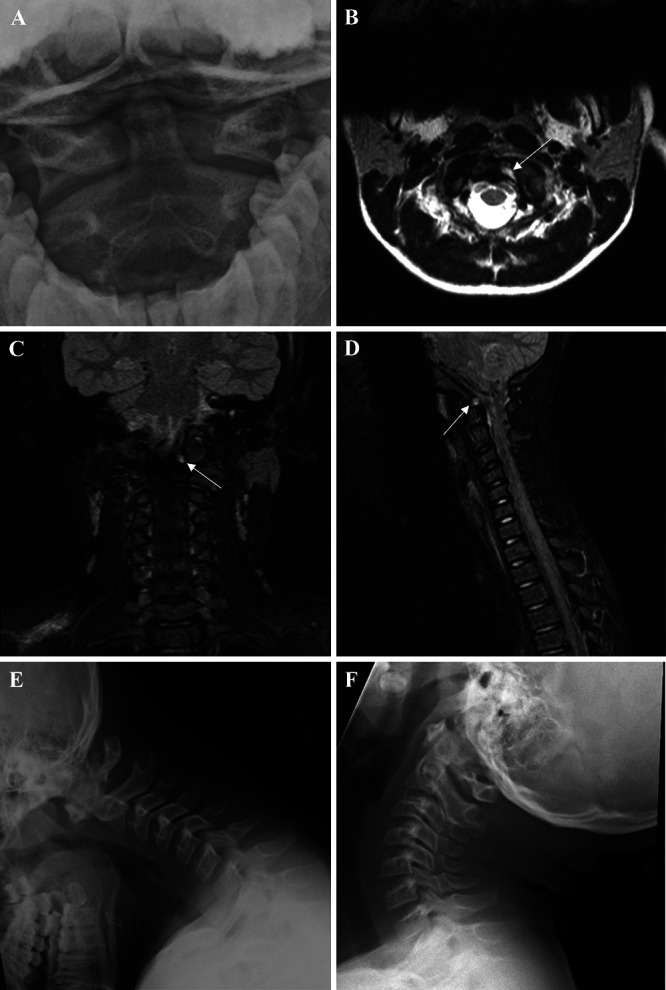
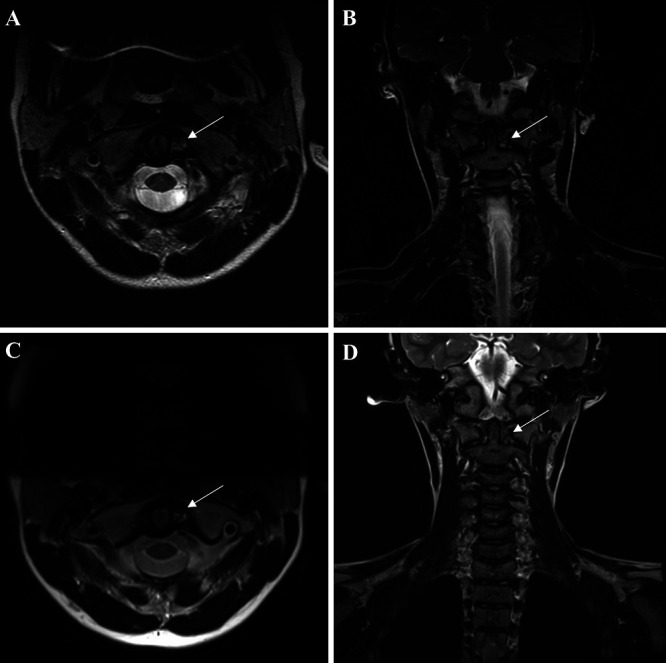
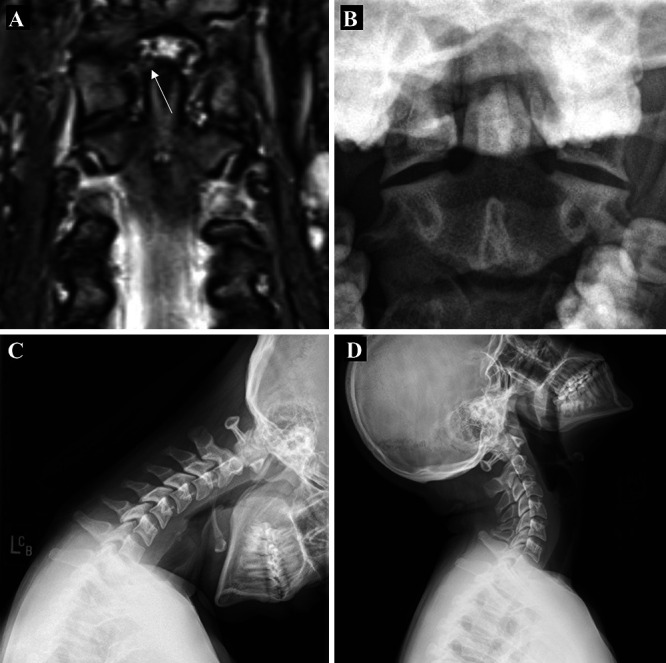
Observations: Here, the authors report on three pediatric patients, each found to have an IUALI after significant trauma. All patients presented with neck tenderness, and two of the three had associated pain-limited range of neck motion. Imaging revealed either a laterally deviated odontoid process on cervical radiographs and/or MRI evidence of ligamentous strain or discontinuity. Each patient was placed in a hard cervical collar for 1 to 2 months with excellent resolution of symptoms. A comprehensive review of the literature showed that all patients with IUALI who had undergone external immobilization with either rigid cervical collar or halo fixation had favorable outcomes at follow-up.
Lessons: For patients with IUALI, a moderate course of nonsurgical management with rigid external immobilization appears to be an adequate first-line treatment.
Keywords: alar ligament; craniocervical junction injury; pediatric; spine trauma.
Conflict of interest statement
Figures
References
-
- Offiah CE. Craniocervical junction and cervical spine anatomy. Neuroimaging Clin N Am. 2022;32(4):875–888. - PubMed
-
- Karray M, M’nif N, Mestiri M, Kooli M, Ezzaouia K, Zlitni M. Concomitant alar and apical ligament avulsion in atlanto-axial rotatory fixation. Case report and review of the literature. Acta Orthop Belg. 2004;70(2):189–192. - PubMed
-
- Pang D, Nemzek WR, Zovickian J. Atlanto-occipital dislocation—part 2: the clinical use of (occipital) condyle-C1 interval, comparison with other diagnostic methods, and the manifestation, management, and outcome of atlanto-occipital dislocation in children. Neurosurgery. 2007;61(5):995–1015. - PubMed
-
- Adams VI. Neck injuries: I. Occipitoatlantal dislocation—a pathologic study of twelve traffic fatalities. J Forensic Sci. 1992;37(2):556–564. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
