

Comparison of early clinical outcome in carpal tunnel release - mini-open technique with palmar incision vs. endoscopic technique with wrist crease incision
- PMID: 38561698
- PMCID: PMC10983724
- DOI: 10.1186/s12891-023-07151-w
Comparison of early clinical outcome in carpal tunnel release - mini-open technique with palmar incision vs. endoscopic technique with wrist crease incision
Abstract
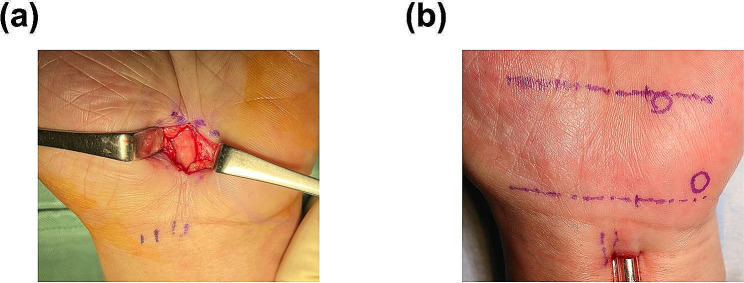
Background: The purpose of this study was to examine two techniques for Carpal Tunnel Syndrome, mini-Open Carpal Tunnel Release (mini-OCTR) and Endoscopic Carpal Tunnel Release (ECTR), to compare their therapeutic efficacy.
Methods: Sixteen patients who underwent mini-OCTR in palmar incision and 17 patients who underwent ECTR in the wrist crease incision were included in the study. All patients presented preoperatively and at 1, 3, and 6 months postoperatively and were assessed with the Visual Analogue Scale (VAS) and the Disabilities of Arm, Shoulder and Hand Score (DASH). We also assessed the pain and cosmetic VAS of the entire affected hand or surgical wound, and the patient's satisfaction with the surgery.
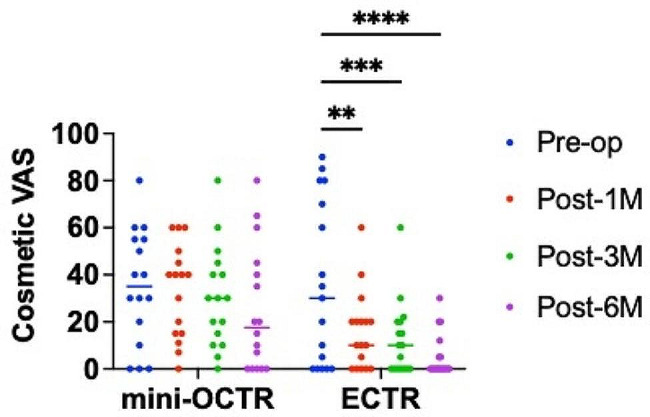
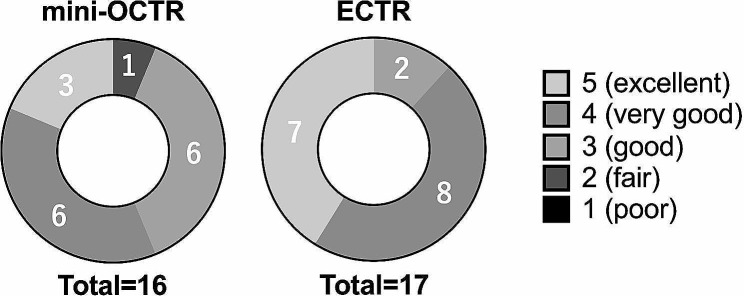
Results: In the objective evaluation, both surgical techniques showed improvement at 6 months postoperatively. The DASH score was significantly lower in the ECTR group (average = 3 months: 13.6, 6 months: 11.9) than in the mini-OCTR group (average = 3 months: 27.3, 6 months: 20.6) at 3 and 6 months postoperatively. Also, the pain VAS score was significantly lower in the ECTR group (average = 17.1) than in the mini-OCTR group (average = 36.6) at 3 months postoperatively. The cosmetic VAS was significantly lower in the ECTR group (average = 1 month: 15.3, 3 months: 12.2, 6 months: 5.41) than in the mini-OCTR group (average = 1 month: 33.3, 3 months: 31.2, 6 months: 24.8) at all time points postoperatively. Patient satisfaction scores tended to be higher in the ECTR group (average = 3.3) compared to the mini-OCTR group (average = 2.7).
Conclusions: ECTR in wrist increase incision resulted in better pain and cosmetic recovery in an early postoperative phase compared with mini-OCTR in palmar incision. Our findings suggest that ECTR is an effective technique for patient satisfaction.
Keywords: Carpal tunnel syndrome; Endoscopy; Mini-open; Patient-oriented evaluation.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
Multistate Comparison of Cost, Trends, and Complications in Open Versus Endoscopic Carpal Tunnel Release.Hand (N Y). 2021 Jan;16(1):25-31. doi: 10.1177/1558944719837020. Epub 2019 Mar 29. Hand (N Y). 2021. PMID: 30924367 Free PMC article.
-
Early Rates of Revision Surgery in Endoscopic and Open Carpal Tunnel Release.J Hand Surg Am. 2025 Jan;50(1):60-69. doi: 10.1016/j.jhsa.2024.09.018. Epub 2024 Nov 16. J Hand Surg Am. 2025. PMID: 39556065
-
Prospective, randomized evaluation of endoscopic versus open carpal tunnel release in bilateral carpal tunnel syndrome: an interim analysis.Ann Plast Surg. 2014 Dec;73 Suppl 2:S157-60. doi: 10.1097/SAP.0000000000000203. Ann Plast Surg. 2014. PMID: 25046667 Clinical Trial.
-
Intraoperative Conversion From Endoscopic to Open Carpal Tunnel Release: A Systematic Review and Case Series.J Hand Surg Am. 2023 Dec;48(12):1244-1251. doi: 10.1016/j.jhsa.2022.06.020. Epub 2022 Aug 13. J Hand Surg Am. 2023. PMID: 35970620
-
Endoscopic Versus Open Carpal Tunnel Release: A Systematic Review of Outcomes and Complications.Cureus. 2024 Jul 20;16(7):e64991. doi: 10.7759/cureus.64991. eCollection 2024 Jul. Cureus. 2024. PMID: 39165434 Free PMC article. Review.
References
-
- Bland JD. Carpal tunnel syndrome. BMJ. 2007;335(7615):343–6. doi: 10.1136/bmj.39282.623553.AD. - DOI - PMC - PubMed
-
- Brown RA, Gelberman RH, Seiler JG 3rd, Abrahamsson SO, Weiland AJ, Urbaniak JR, Schoenfeld DA, Furcolo D. Carpal tunnel release. A prospective, randomized assessment of open and endoscopic methods. J Bone Joint Surg Am. 1993;75(9):1265–75. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
